

Anifrolumab in lupus nephritis: results from second-year extension of a randomised phase II trial
- PMID: 37607780
- PMCID: PMC10445374
- DOI: 10.1136/lupus-2023-000910
Anifrolumab in lupus nephritis: results from second-year extension of a randomised phase II trial
Abstract
Objective: To characterise the safety and efficacy of anifrolumab in active lupus nephritis (LN) through year 2 of the phase II randomised, double-blind Treatment of Uncontrolled Lupus via the Interferon Pathway (TULIP)-LN trial (NCT02547922) of 2 anifrolumab dosing regimens versus placebo.
Methods: Patients received intravenous anifrolumab 900 mg for the first 3 doses followed by 300 mg anifrolumab (intensified regimen (IR)), 300 mg anifrolumab (basic regimen (BR)) or placebo every 4 weeks throughout. To continue into Year 2, patients must have achieved at least partial renal response and a glucocorticoid tapering target.
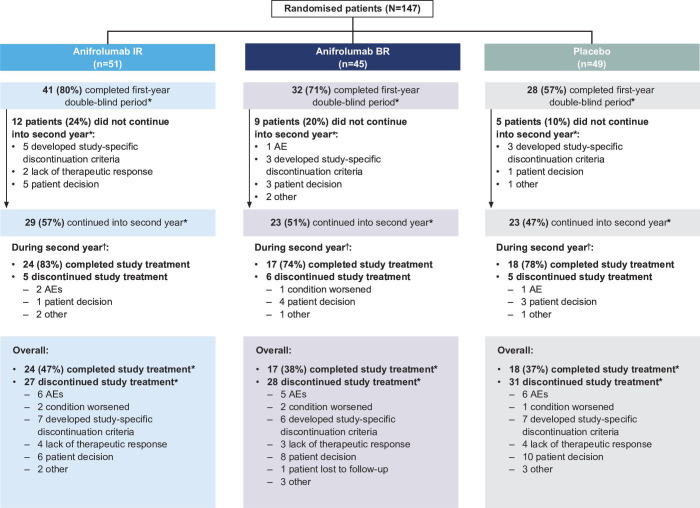
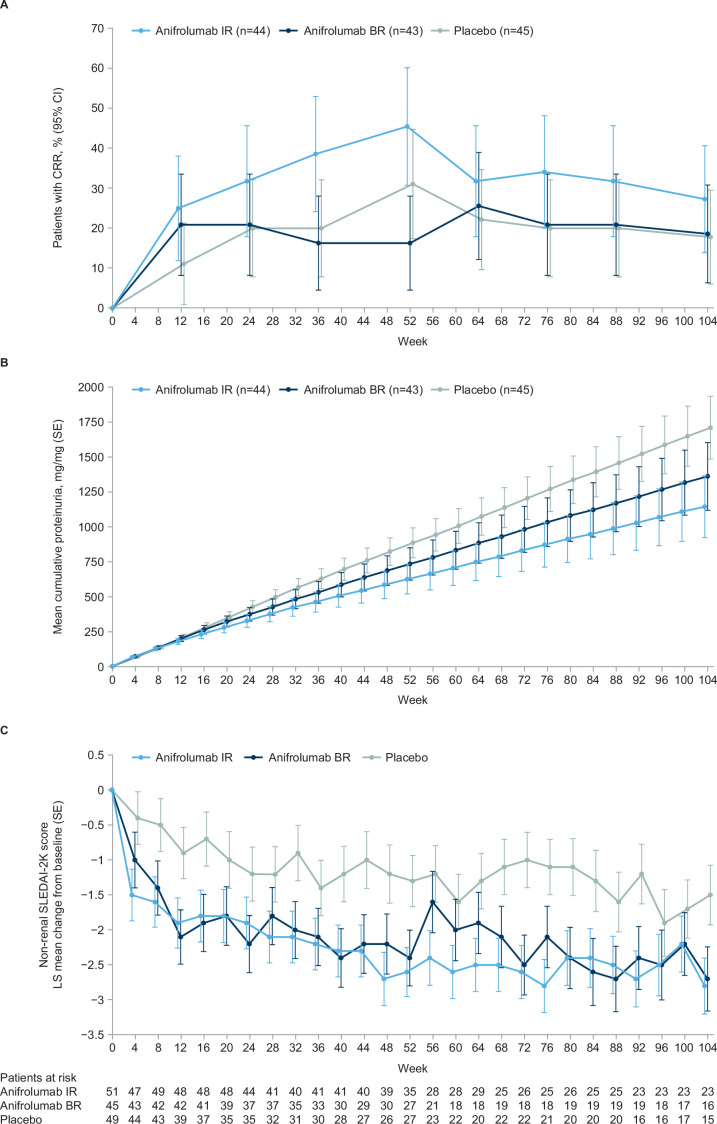
Results: Of 147 randomised patients, 101 completed Year 1 study treatment; of these, 75 (74%) continued into Year 2 (anifrolumab IR: n=29, BR: n=23 and placebo: n=23). During Year 2, 72% of patients reported ≥1 adverse event (AE); serious AEs were reported in 6.9%, 8.7% and 8.7% of patients (anifrolumab IR, BR and placebo, respectively); 3 patients discontinued treatment due to an AE (anifrolumab IR: n=2 and placebo: n=1) and herpes zoster was reported in 2 patients (anifrolumab IR: n=1 and BR: n=1). The study was ongoing at the start of the pandemic, but no COVID-19 cases were reported. Of the 145 patients receiving treatment, more patients on the IR attained complete renal response at Week 104 compared with those on BR or placebo (27.3% vs 18.6% and 17.8%) and simultaneously achieved sustained glucocorticoid tapering (IR: 25.0%; BR: 18.6% and placebo: 17.8%). The improvements in estimated glomerular filtration rate were numerically larger in both anifrolumab groups versus placebo.
Conclusions: The safety and tolerability profile through Year 2 of TULIP-LN was generally consistent with Year 1, with promising efficacy results for the anifrolumab IR regimen. Collectively, the results support further investigation of an anifrolumab intensified dosing regimen in larger populations of patients with active proliferative LN.
Trial registration number: NCT02547922.
Keywords: autoimmune diseases; lupus nephritis; therapeutics.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: DJ has received consulting fees from Boehringer Ingelheim, Chemocentryx, CSL Vifor, Novartis, Roche and Takeda; has received honoraria from CSL Vifor and GSK; has received payment for participating in Data Safety Monitoring or Advisory Boards for Chinook, GSK and Takeda and has stock or stock options in Aurinia. BR has received consulting fees from Aurinia, Alexion, AstraZeneca, Biocryst, Biogen, BMS, Calliditas, Chemocentryx, Corrona, EMD Serono, Exagen, Galapagos, Genentech-Roche, GSK, Janssen, Kezar, Lilly, MorphoSys, Novartis, Omeros, Otsuka, Pfizer, Travere and University of Minnesota; has received speaker support from the American Society of Nephrology and the International Society of Nephrology and has a leadership or fiduciary role in the Lupus Foundation of America and KDIGO Glomerulonephritis Guideline group. EM has received grants or contracts from AbbVie, AstraZeneca, BMS, Janssen, Lilly, Novartis, Pfizer and Roche; has received consulting fees from AbbVie, AstraZeneca, GSK, Janssen, Lilly and Pfizer; has received honoraria from AbbVie, Amgen, AstraZeneca, GSK, Janssen, Lilly, Pfizer and Sanofi; has received payment for expert testimony from AbbVie and has received support for attending meetings and/or travel from AbbVie and Pfizer. RF has received consulting fees, payment or honoraria for speaking, support for attending meetings from and payment for participating in a Data Safety Monitoring or Advisory Board for AstraZeneca. FH has received grants or contracts from GSK and consulting fees from IDORSIA. RT is an employee of AstraZeneca. TT, JK, ES, WT and CL are employees of AstraZeneca and own stock or stock options.
Figures
References
-
- Fanouriakis A, Kostopoulou M, Cheema K, et al. . 2019 Update of the joint European League Against Rheumatism and European Renal Association-European Dialysis and Transplant Association (EULAR/ERA-EDTA) recommendations for the management of lupus nephritis. Ann Rheum Dis 2020;79:713–23. 10.1136/annrheumdis-2020-216924 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical