

Influence of knee flexion angle on graft bending angle during anterior cruciate ligament reconstruction using the transportal technique
- PMID: 37608212
- PMCID: PMC10444777
- DOI: 10.1038/s41598-023-41002-x
Influence of knee flexion angle on graft bending angle during anterior cruciate ligament reconstruction using the transportal technique
Abstract
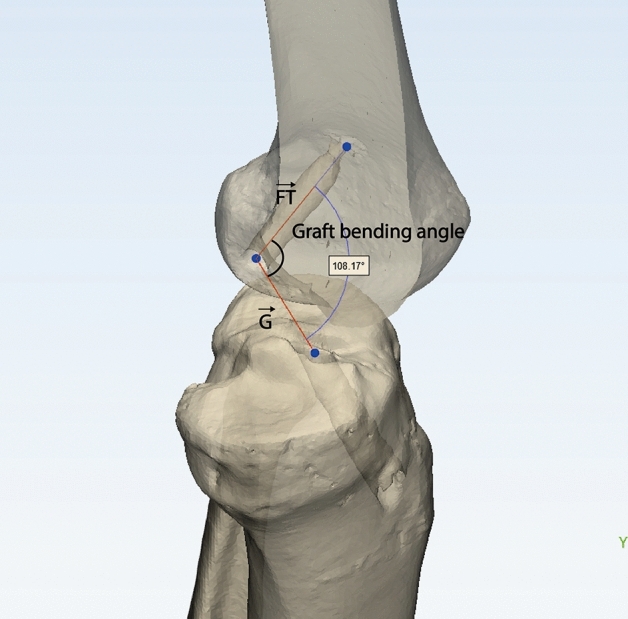
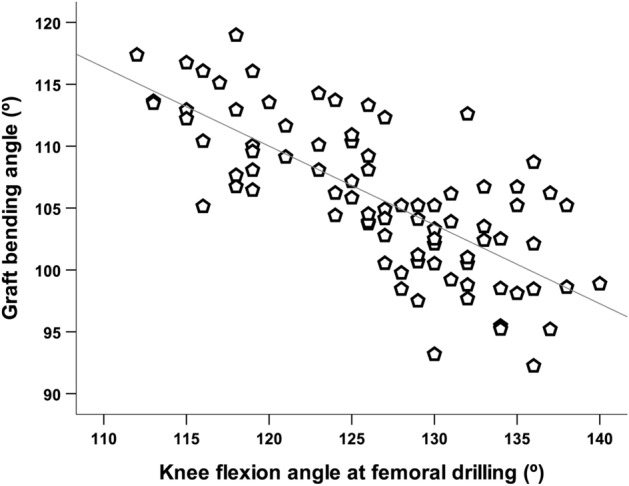
This study aimed to examine change in the graft bending angle (GBA) according to various knee flexion angles in creating femoral tunnel by the transportal technique in ACL reconstruction, and to reveal knee flexion angle minimizing GBA while maintaining stable femoral tunnel characteristics. Patients who underwent ACL reconstruction using the transportal technique between January 2017 and December 2018 were retrospectively reviewed. Patients were classified into three groups according to knee flexion angle when creating femoral tunnel (group 1: < 120° (n = 19); group 2: 120-129° (n = 32); group 3: ≥ 130° (n = 33). GBA was measured on three-dimensional knee model reconstructed from postoperative computed tomography images. The length of the femoral tunnel and posterior wall blow-out were also checked. There was significant difference of GBA between the groups (group 1 = 112.1°; group 2 = 106.4°; group 3 = 101.4°, p < 0.001). The knee flexion angle in creating femoral tunnel was negatively correlated with GBA (r = - 0.733, p < 0.001). Five patients in group 1 had short femoral tunnel. GBA was influenced by knee flexion angle in creating femoral tunnel and got more acute as the knee flexion angle increased. Considering length and risk of wall blow-out in femoral tunnel, and GBA, knee flexion angle between 120 and 130° could be recommended as appropriate angle to create optimal femoral tunnel in ACL reconstruction using the transportal technique.
© 2023. Springer Nature Limited.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Does Knee Flexion Influence the Relationship between the Femoral Tunnel and the Lateral Anatomic Structures During ACL Reconstruction?Clin Orthop Relat Res. 2019 Oct;477(10):2228-2239. doi: 10.1097/CORR.0000000000000845. Clin Orthop Relat Res. 2019. PMID: 31169629 Free PMC article.
-
Shallow knee flexion angle during femoral tunnel creation using modified transtibial technique can reduce femoral graft bending angle in ACL reconstruction.Knee Surg Sports Traumatol Arthrosc. 2019 Feb;27(2):618-625. doi: 10.1007/s00167-018-5191-0. Epub 2018 Oct 9. Knee Surg Sports Traumatol Arthrosc. 2019. PMID: 30302534
-
Influence of knee flexion angle and transverse drill angle on creation of femoral tunnels in double-bundle anterior cruciate ligament reconstruction using the transportal technique: Three-dimensional computed tomography simulation analysis.Knee. 2018 Jan;25(1):99-108. doi: 10.1016/j.knee.2017.09.005. Epub 2017 Oct 1. Knee. 2018. PMID: 28978459
-
In Vivo Analysis of Dynamic Graft Bending Angle in Anterior Cruciate Ligament-Reconstructed Knees During Downward Running and Level Walking: Comparison of Flexible and Rigid Drills for Transportal Technique.Arthroscopy. 2017 Jul;33(7):1393-1402. doi: 10.1016/j.arthro.2017.01.041. Epub 2017 Mar 24. Arthroscopy. 2017. PMID: 28343809 Free PMC article.
-
Medial portal drilling: effects on the femoral tunnel aperture morphology during anterior cruciate ligament reconstruction.J Bone Joint Surg Am. 2011 Nov 16;93(22):2063-71. doi: 10.2106/JBJS.J.01705. J Bone Joint Surg Am. 2011. PMID: 22262377 Review.
Cited by
-
High flexion femoral side remnant preservation positioning technique: a new method for positioning the femoral tunnel in anterior cruciate ligament reconstruction.J Orthop Surg Res. 2024 Mar 18;19(1):189. doi: 10.1186/s13018-024-04670-7. J Orthop Surg Res. 2024. PMID: 38500214 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
