

Mediastinal Intrathymic Parathyroid Adenoma: A Case Report and Review of the Literature
- PMID: 37609099
- PMCID: PMC10442188
- DOI: 10.7759/cureus.42306
Mediastinal Intrathymic Parathyroid Adenoma: A Case Report and Review of the Literature
Abstract
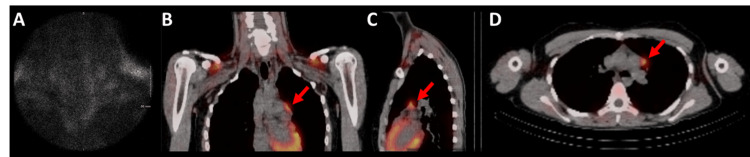
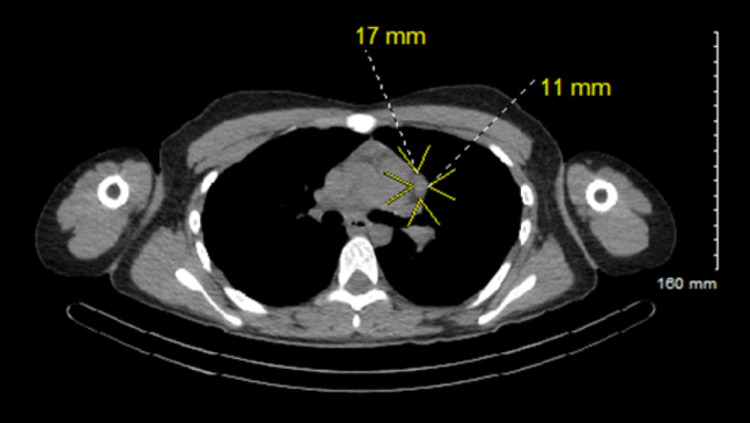
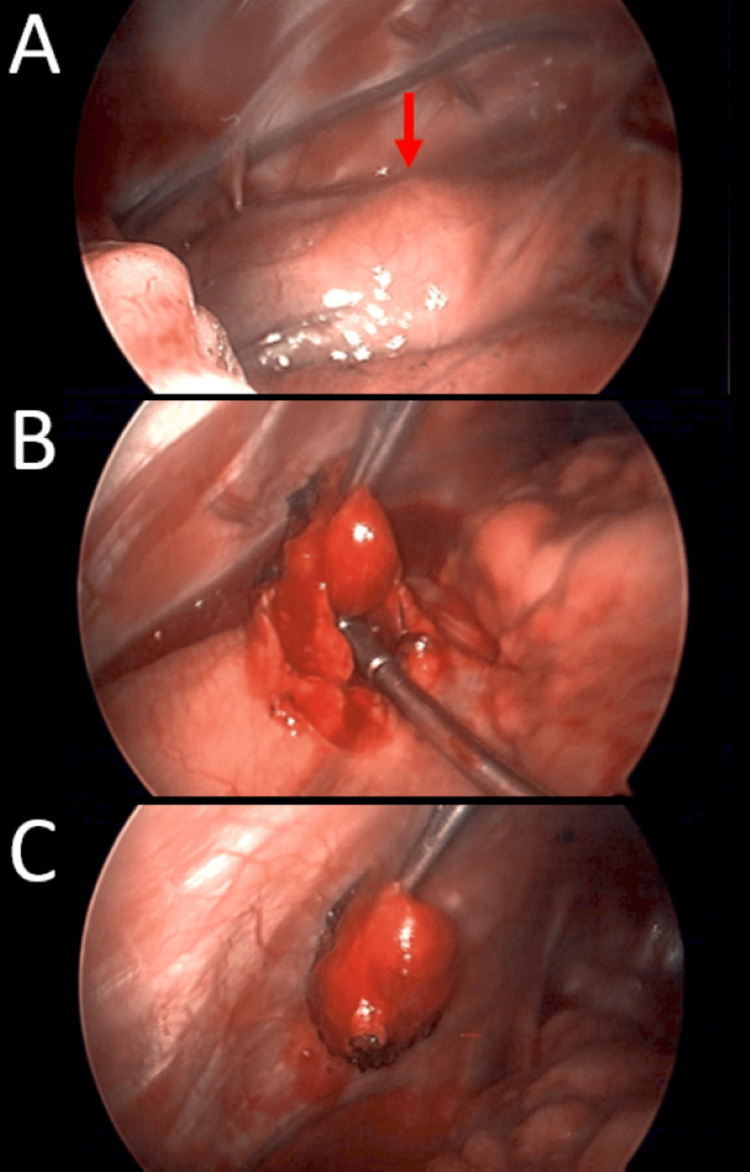
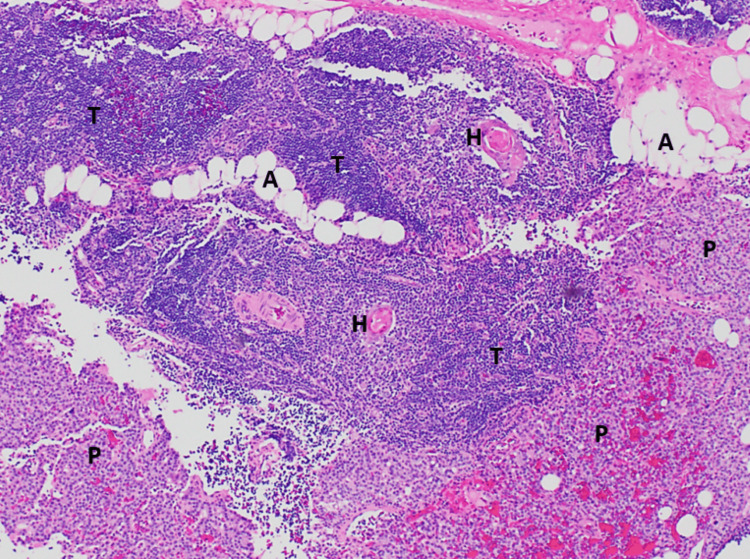
The classic clinical vignette of primary hyperparathyroidism is well described as "bones, stones, abdominal moans, and psychiatric overtones" to reflect the effects of excess parathyroid hormone (PTH) and calcium. Most commonly, primary hyperparathyroidism is due to a functional parathyroid adenoma situated by the thyroid gland. Rarely, the primary focus of autonomously produced PTH is located ectopically within the mediastinum. A 19-year-old Caucasian female with no relevant past medical history presented to the emergency department with tachycardia, nausea, vomiting, and a five-day history of vague, mid-abdominal pain. Initial computed tomography (CT) with contrast of the abdomen and pelvis was negative for acute findings, and she subsequently underwent biochemical screening. The patient was found to have elevated serum calcium and PTH, raising suspicion for the diagnosis of primary hyperparathyroidism. Further evaluation for a parathyroid adenoma was negative by a CT scan of the neck and thyroid ultrasound. A nuclear medicine parathyroid single-photon emission computed tomography (SPECT)/CT with technetium (Tc) 99m sestamibi found an abnormal nodular uptake within the left prevascular mediastinum suggestive of an ectopic parathyroid adenoma. A left-sided, video-assisted thoracoscopic surgery (VATS) with successful excision of the ectopic mediastinal parathyroid adenoma was performed. Surgical pathology revealed that the parathyroid adenoma was completely excised and surrounded by thymus and adipose tissue. The patient tolerated the procedure well and was discharged without further complications. The rarity of mediastinal, intrathymic parathyroid adenomas resulted in delayed diagnosis in this patient, understandably so as errant embryogenesis does not occur commonly. Visualization with SPECT/CT and successful specimen excision by minimally invasive VATS resulted in the accurate diagnosis and ultimate cure of this patient's primary hyperparathyroidism.
Keywords: ectopic parathyroid tissue; hypercalcemia; hyperparathyroid; intra-thymic; solitary parathyroid adenoma; spect-ct; video-assisted thoracoscopic surgery (vats).
Copyright © 2023, Abraham et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Hyperparathyroidism. Fraser WD. Lancet. 2009;374:145–158. - PubMed
-
- A systematic review of the diagnosis and treatment of primary hyperparathyroidism from 1995 to 2003. Ruda JM, Hollenbeak CS, Stack BC Jr. Otolaryngol Head Neck Surg. 2005;132:359–372. - PubMed
-
- Update in parathyroid imaging. Kuzminski SJ, Sosa JA, Hoang JK. Magn Reson Imaging Clin N Am. 2018;26:151–166. - PubMed
-
- Pradhan R, Agarwal A, Lombardi CP, Raffaelli M. Surgery of the Thyroid and Parathyroid Glands. Philadelphia, PA: Saunders/Elsevier; 2013. Applied embryology of the thyroid and parathyroid glands.
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous