

Sex Differences in Clinical Characteristics and Outcomes After Myocardial Infarction With Low Ejection Fraction: Insights From PARADISE-MI
- PMID: 37609931
- PMCID: PMC10547323
- DOI: 10.1161/JAHA.122.028942
Sex Differences in Clinical Characteristics and Outcomes After Myocardial Infarction With Low Ejection Fraction: Insights From PARADISE-MI
Abstract
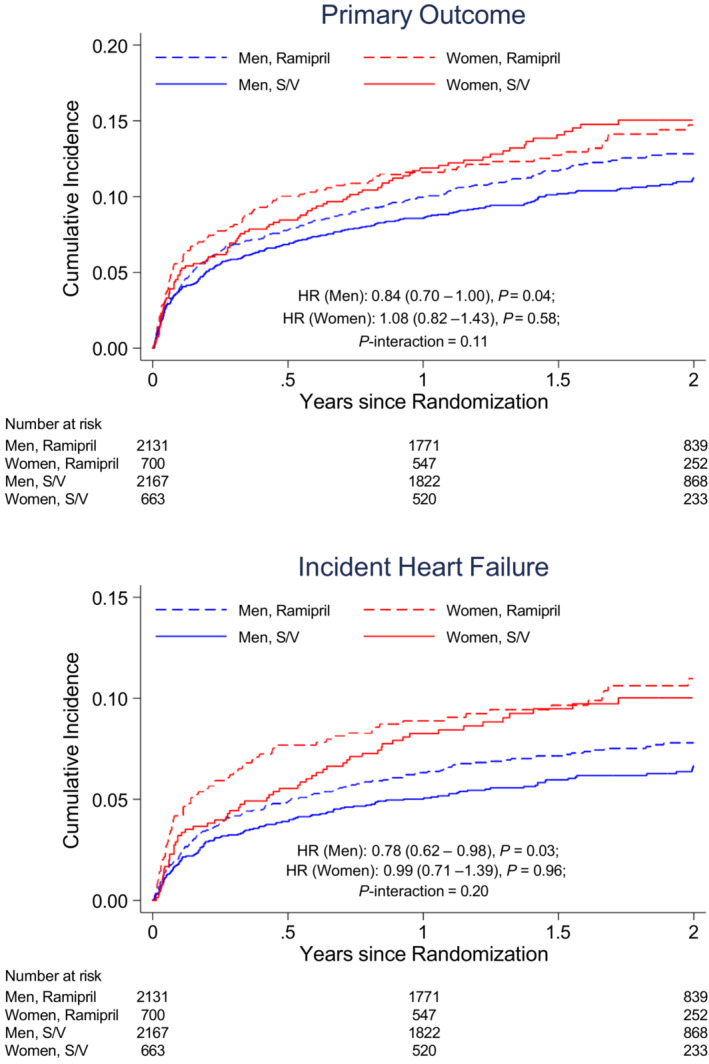
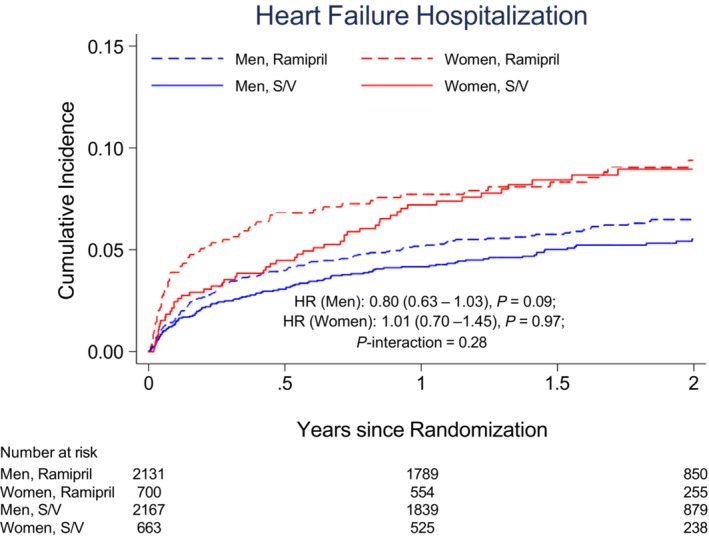
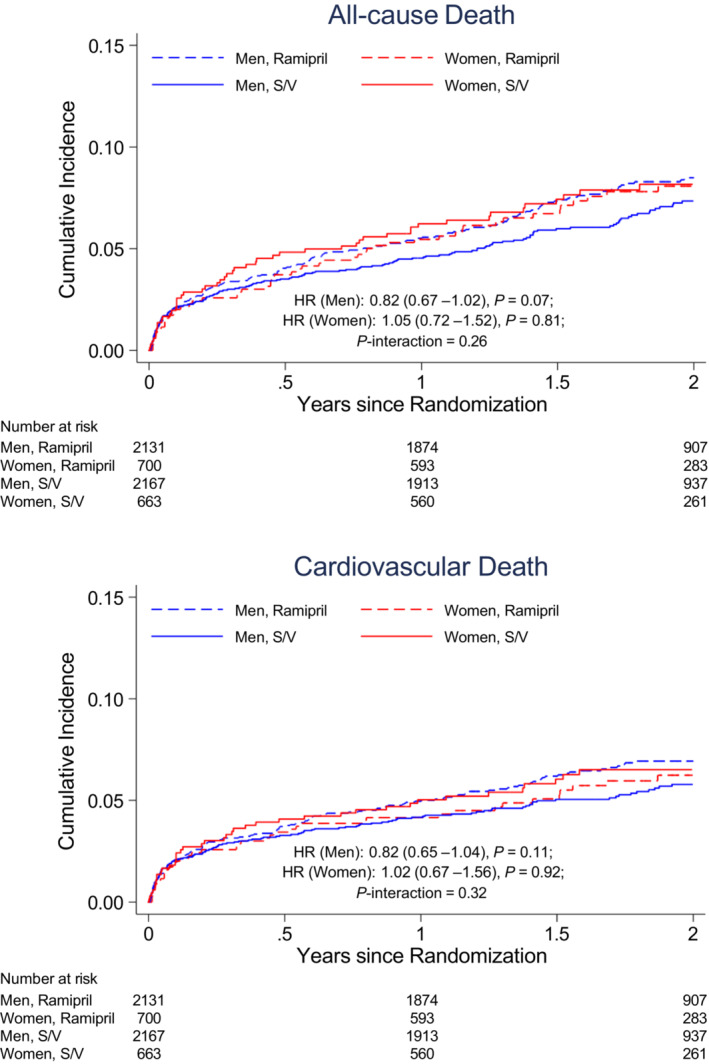
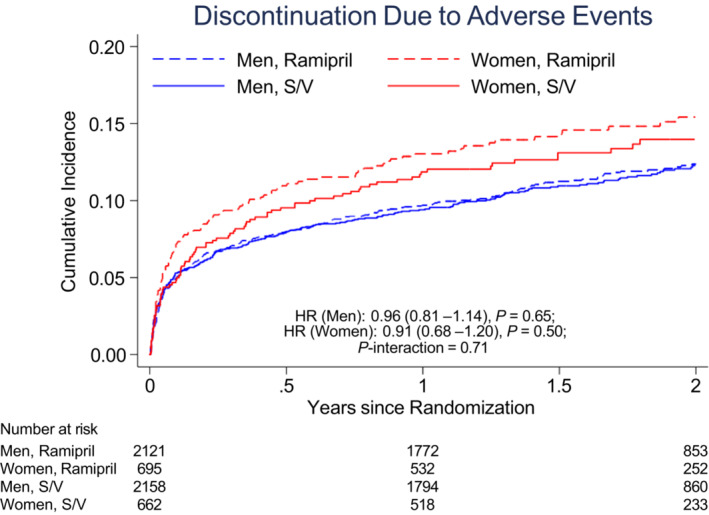
Background Studies demonstrated sex differences in outcomes following acute myocardial infarction, with women more likely to develop heart failure (HF). Sacubitril/valsartan has been shown to reduce cardiovascular death and HF hospitalizations in patients with HF with reduced ejection fraction. Methods and Results A total of 5661 patients (1363 women [24%]) with acute myocardial infarction complicated by reduced left ventricular ejection fraction (≤40%), pulmonary congestion, or both and ≥1 of 8 risk-augmenting factors were randomized to receive sacubitril/valsartan or ramipril. The primary outcome was cardiovascular death or incident HF. Baseline characteristics, clinical outcomes, and safety events were compared according to sex, a prespecified subgroup. Female participants were older and had more comorbidities. After multivariable adjustment, women and men were at similar risks for cardiovascular death or all-cause death. Women were more likely to have first HF hospitalization (hazard ratio [HR], 1.34 [95% CI, 1.05-1.70]; P=0.02) and total HF hospitalizations (HR, 1.39 [95% CI, 1.05-1.84]; P=0.02). Sex did not significantly modify the treatment effect of sacubitril/valsartan compared with ramipril on the primary outcome (P for interaction=0.11). Conclusions In contemporary patients who presented with reduced left ventricular ejection fraction, pulmonary congestion, or both, following acute myocardial infarction, women had a higher incidence of HF during follow-up. Sex did not modify the treatment effect of sacubitril/valsartan relative to ramipril. Registration URL: https://www.clinicaltrials.gov; Unique identifier: NCT02924727.
Keywords: heart failure; myocardial infarction; sacubitril/valsartan; sex differences.
Figures
References
-
- Blomkalns AL, Chen AY, Hochman JS, Peterson ED, Trynosky K, Diercks DB, Brogan GX Jr, Boden WE, Roe MT, Ohman EM, et al. Gender disparities in the diagnosis and treatment of non‐ST‐segment elevation acute coronary syndromes: large‐scale observations from the CRUSADE (can rapid risk stratification of unstable angina patients suppress adverse outcomes with early implementation of the American College of Cardiology/American Heart Association guidelines) National Quality Improvement Initiative. J Am Coll Cardiol. 2005;45:832–837. doi: 10.1016/j.jacc.2004.11.055 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
