

Elevation of IL-17 Cytokines Distinguishes Kawasaki Disease From Other Pediatric Inflammatory Disorders
- PMID: 37610270
- PMCID: PMC10842426
- DOI: 10.1002/art.42680
Elevation of IL-17 Cytokines Distinguishes Kawasaki Disease From Other Pediatric Inflammatory Disorders
Abstract
Objective: Kawasaki disease (KD) is a systemic vasculitis of young children that can lead to development of coronary artery aneurysms. We aimed to identify diagnostic markers to distinguish KD from other pediatric inflammatory diseases.
Methods: We used the proximity extension assay to profile proinflammatory mediators in plasma samples from healthy pediatric controls (n = 30), febrile controls (n = 26), and patients with KD (n = 23), multisystem inflammatory syndrome in children (MIS-C; n = 25), macrophage activation syndrome (n = 13), systemic and nonsystemic juvenile idiopathic arthritis (n = 14 and n = 10, respectively), and juvenile dermatomyositis (n = 9). We validated the key findings using serum samples from additional patients with KD (n = 37) and febrile controls (n = 28).
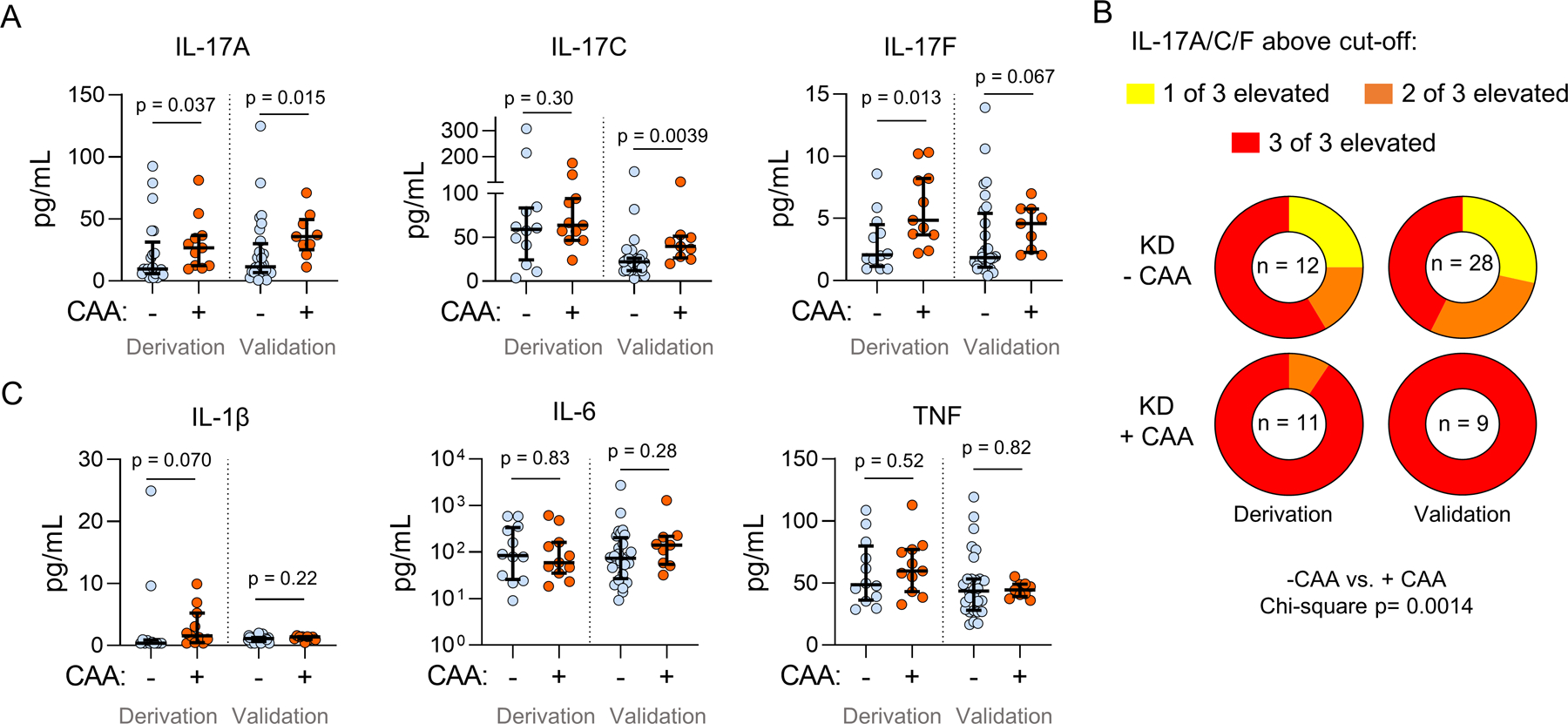
Results: High-fidelity proteomic profiling revealed distinct patterns of cytokine and chemokine expression across pediatric inflammatory diseases. Although KD and MIS-C exhibited many similarities, KD differed from MIS-C and other febrile diseases in that most patients exhibited elevation in one or more members of the interleukin-17 (IL-17) cytokine family, IL-17A, IL-17C, and IL-17F. IL-17A was particularly sensitive and specific, discriminating KD from febrile controls with an area under the receiver operator characteristic curve of 0.95 (95% confidence interval 0.89-1.00) in the derivation set and 0.91 (0.85-0.98) in the validation set. Elevation of all three IL-17-family cytokines was observed in over 50% of KD patients, including 19 of 20 with coronary artery aneurysms, but was rare in all other comparator groups.
Conclusion: Elevation of IL-17 family cytokines is a hallmark of KD and may help distinguish KD from its clinical mimics.
© 2023 American College of Rheumatology.
Conflict of interest statement
Conflict of interest statement:
The authors declare the following conflicts of interest related to this work:
FD is a consultant for Novartis and receives royalties from UpToDate.
AD receives sponsored research funding from Pfizer.
SDF receives royalties from UpToDate.
LAH is a consultant for Adaptive Biotech, Pfizer, and Sobi, receives sponsored research funding from BMS, and receives royalties from CARRA.
PAN is a consultant for BMS, Fresh Track Therapeutics, Exo Therapeutics, Merck, Novartis, Pfizer, Qiagen, and Sobi, receives sponsored research from BMS and Pfizer, and receives royalties from the American Academy of Pediatrics and UpToDate.
MBS receives royalties from UpToDate.
JWN receives sponsored research from Pfizer and BMS and receives royalties from UpToDate.
PYL is a consultant for Fresh Track Therapeutics and Exo Therapeutics and receives royalties from UpToDate.
The other authors declare no conflict of interest.
Figures


References
-
- McCrindle BW, Rowley AH, Newburger JW, Burns JC, Bolger AF, Gewitz M, et al. Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease: A Scientific Statement for Health Professionals From the American Heart Association. Circulation 2017;135(17):e927–e99. - PubMed
-
- Newburger JW, Takahashi M, Burns JC, Beiser AS, Chung KJ, Duffy CE, et al. The treatment of Kawasaki syndrome with intravenous gamma globulin. N Engl J Med 1986;315(6):341–7. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
