

Early Evidence of Chronic Obstructive Pulmonary Disease Obscured by Race-Specific Prediction Equations
- PMID: 37611073
- PMCID: PMC10870894
- DOI: 10.1164/rccm.202303-0444OC
Early Evidence of Chronic Obstructive Pulmonary Disease Obscured by Race-Specific Prediction Equations
Abstract
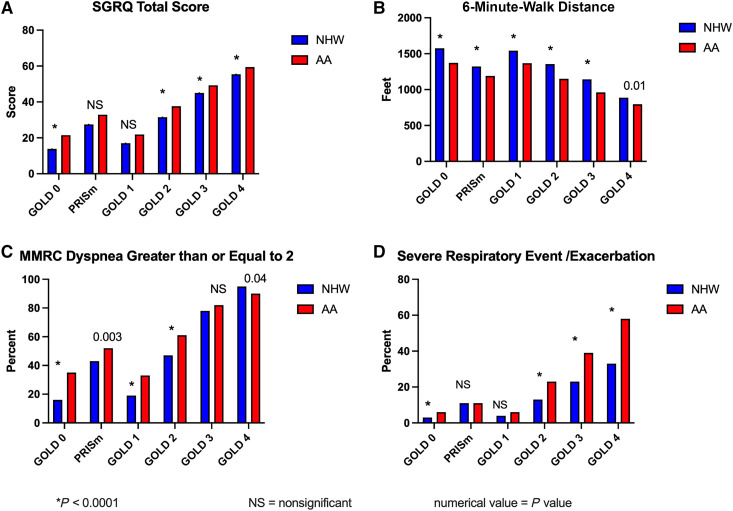
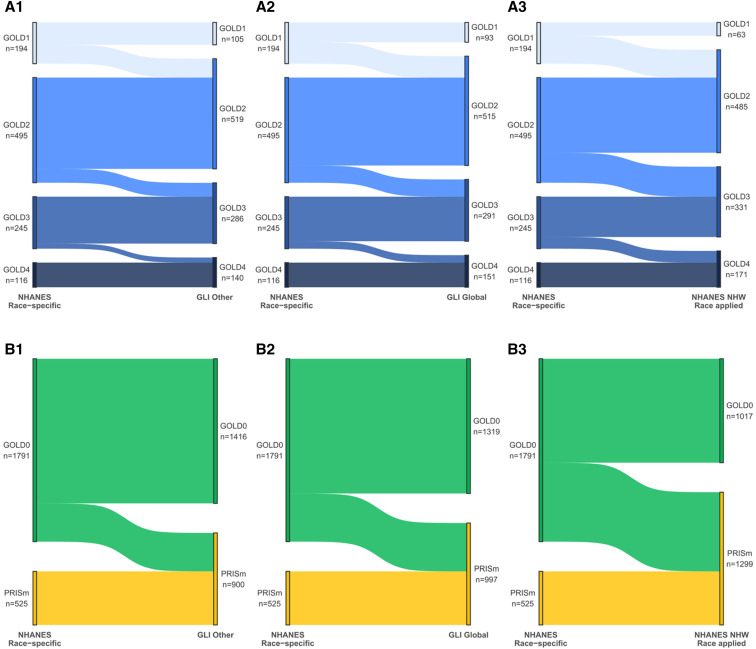
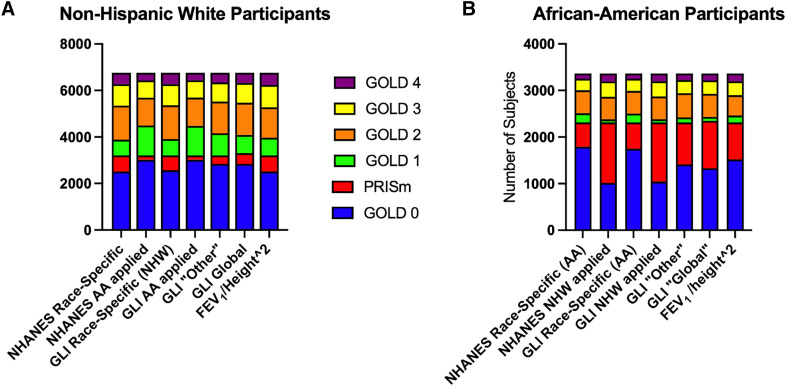
Rationale: The identification of early chronic obstructive pulmonary disease (COPD) is essential to appropriately counsel patients regarding smoking cessation, provide symptomatic treatment, and eventually develop disease-modifying treatments. Disease severity in COPD is defined using race-specific spirometry equations. These may disadvantage non-White individuals in diagnosis and care. Objectives: Determine the impact of race-specific equations on African American (AA) versus non-Hispanic White individuals. Methods: Cross-sectional analyses of the COPDGene (Genetic Epidemiology of Chronic Obstructive Pulmonary Disease) cohort were conducted, comparing non-Hispanic White (n = 6,766) and AA (n = 3,366) participants for COPD manifestations. Measurements and Main Results: Spirometric classifications using race-specific, multiethnic, and "race-reversed" prediction equations (NHANES [National Health and Nutrition Examination Survey] and Global Lung Function Initiative "Other" and "Global") were compared, as were respiratory symptoms, 6-minute-walk distance, computed tomography imaging, respiratory exacerbations, and St. George's Respiratory Questionnaire. Application of different prediction equations to the cohort resulted in different classifications by stage, with NHANES and Global Lung Function Initiative race-specific equations being minimally different, but race-reversed equations moving AA participants to more severe stages and especially between the Global Initiative for Chronic Obstructive Lung Disease (GOLD) stage 0 and preserved ratio impaired spirometry groups. Classification using the established NHANES race-specific equations demonstrated that for each of GOLD stages 1-4, AA participants were younger, had fewer pack-years and more current smoking, but had more exacerbations, shorter 6-minute-walk distance, greater dyspnea, and worse BODE (body mass index, airway obstruction, dyspnea, and exercise capacity) scores and St. George's Respiratory Questionnaire scores. Differences were greatest in GOLD stages 1 and 2. Race-reversed equations reclassified 774 AA participants (43%) from GOLD stage 0 to preserved ratio impaired spirometry. Conclusions: Race-specific equations underestimated disease severity among AA participants. These effects were particularly evident in early disease and may result in late detection of COPD.
Keywords: COPD; dyspnea; early disease; health inequities; race-specific spirometry prediction equations.
Figures
Comment in
-
Truth and Consequences: Choosing the Best Interpretative Framework for Spirometry.Am J Respir Crit Care Med. 2024 Jan 1;209(1):6-7. doi: 10.1164/rccm.202308-1493ED. Am J Respir Crit Care Med. 2024. PMID: 37699143 Free PMC article. No abstract available.
References
-
- Safiri S, Carson-Chahhoud K, Noori M, Nejadghaderi SA, Sullman MJM, Ahmadian Heris J, et al. Burden of chronic obstructive pulmonary disease and its attributable risk factors in 204 countries and territories, 1990–2019: results from the Global Burden of Disease Study 2019. BMJ . 2022;378:e069679. - PMC - PubMed
-
- Adeloye D, Song P, Zhu Y, Campbell H, Sheikh A, Rudan I, NIHR RESPIRE Global Respiratory Health Unit Global, regional, and national prevalence of, and risk factors for, chronic obstructive pulmonary disease (COPD) in 2019: a systematic review and modelling analysis. Lancet Respir Med . 2022;10:447–458. - PMC - PubMed
-
- Schluger NW, Dozor AJ, Jung YEG. Rethinking the race adjustment in pulmonary function testing. Ann Am Thorac Soc . 2022;19:353–356. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
