

Complications and failure-to-rescue after pancreatectomy and hospital participation in the targeted American College of Surgeons National Surgical Quality Improvement Program registry
- PMID: 37612210
- PMCID: PMC10592020
- DOI: 10.1016/j.surg.2023.07.023
Complications and failure-to-rescue after pancreatectomy and hospital participation in the targeted American College of Surgeons National Surgical Quality Improvement Program registry
Abstract
Background: More than 700 hospitals participate in the American College of Surgeons National Surgical Quality Improvement Program, but most pancreatectomies are performed in 165 centers participating in the pancreas procedure-targeted registry. We hypothesized that these hospitals ("targeted hospitals") might provide more specialized care than those not participating ("standard hospitals").
Methods: The 2014 to 2019 pancreas-targeted and standard American College of Surgeons National Surgical Quality Improvement Program registry were reviewed regarding patient demographics, comorbidities, and perioperative outcomes using standard univariate and multivariable logistic regression analyses. Primary outcomes included 30-day mortality and serious morbidity.
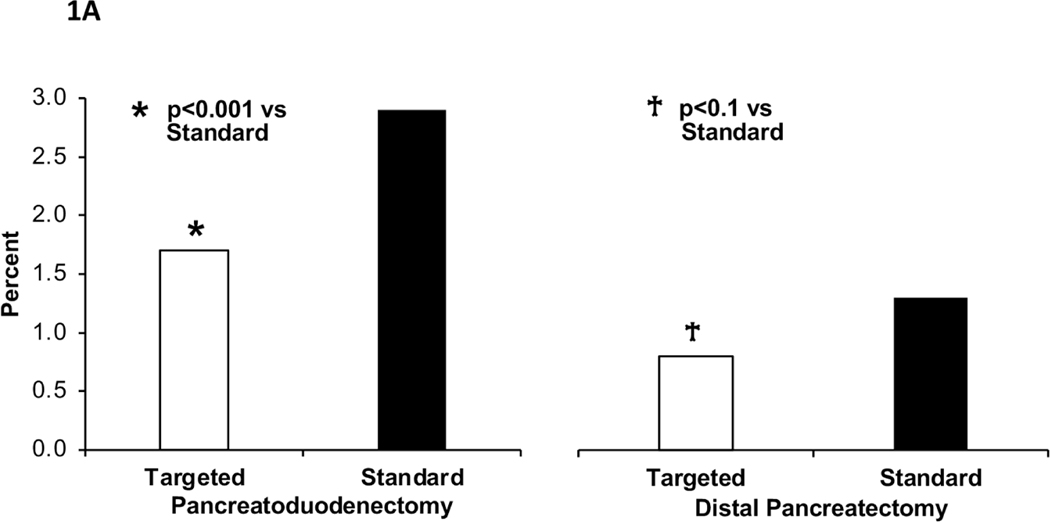
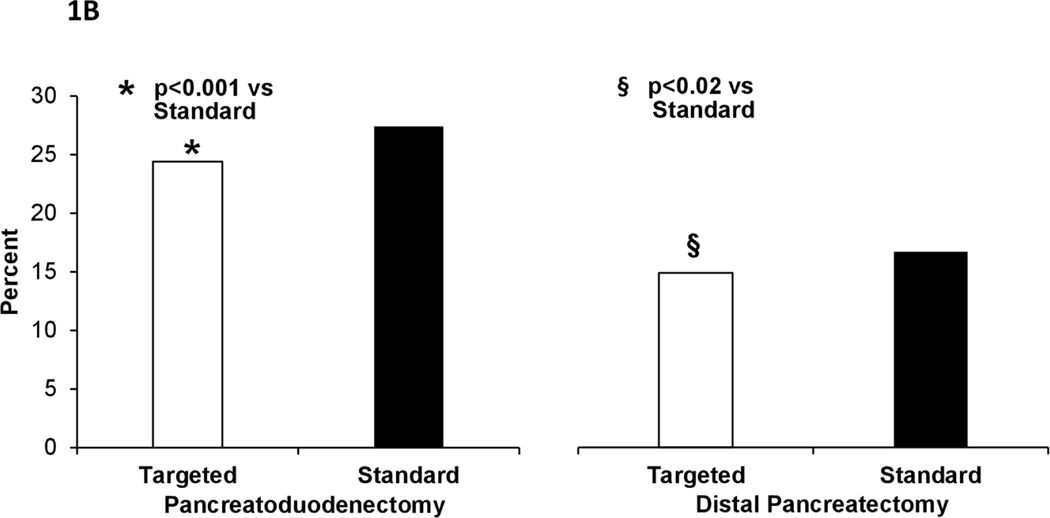
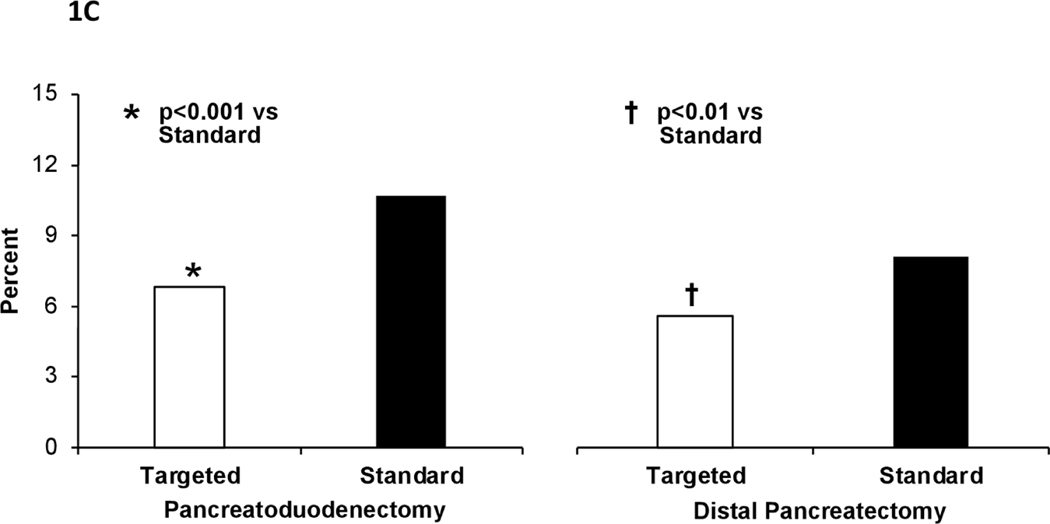
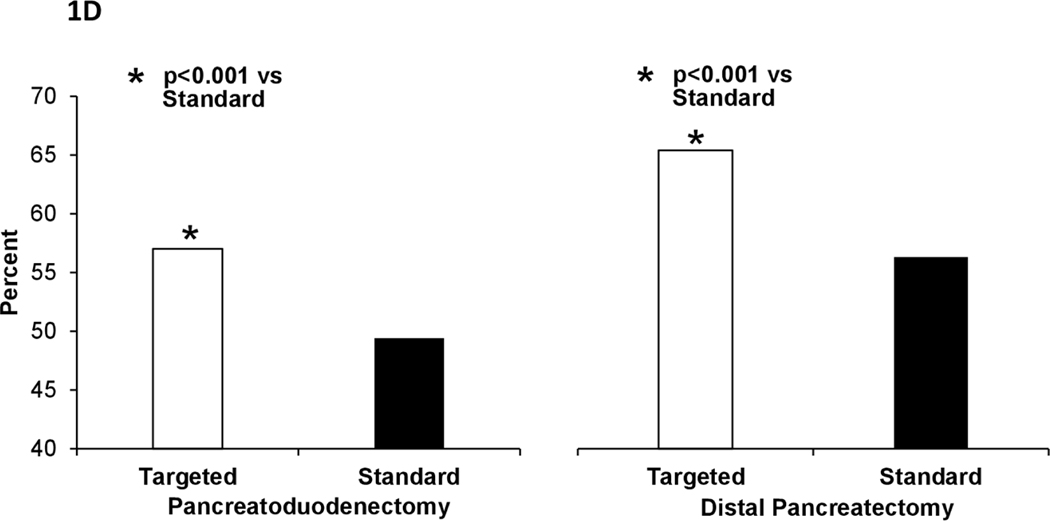
Results: The registry included 30,357 pancreatoduodenectomies (80% in targeted hospitals) and 14,800 distal pancreatectomies (76% in targeted hospitals). Preoperative and intraoperative characteristics of patients treated at targeted versus standard hospitals were comparable. On multivariable analysis, pancreatoduodenectomies performed at targeted hospitals were associated with a 39% decrease in 30-day mortality (odds ratio, 0.61; 95% confidence interval, 0.50-0.75), 17% decrease in serious morbidity (odds ratio, 0.83; 95% confidence interval, 0.77-0.89), and 41% decrease in failure-to-rescue (odds ratio, 0.59; 95% confidence interval, 0.47-0.74). These differences did not apply to distal pancreatectomies. Participation in the targeted registry was associated with higher rates of optimal surgery for both pancreatoduodenectomy (odds ratio, 1.33; 95% confidence interval, 1.25-1.41) and distal pancreatectomy (odds ratio, 1.17; 95% confidence interval, 1.06-1.30).
Conclusion: Mortality and failure-to-rescue rates after pancreatoduodenectomy in targeted hospitals were nearly half of rates in standard American College of Surgeons National Surgical Quality Improvement Program hospitals. Further research should delineate factors underlying this effect and highlight opportunities for improvement.
Copyright © 2023 Elsevier Inc. All rights reserved.
Conflict of interest statement
CONFLICT OF INTEREST/DISCLOSURE
The authors have no relevant financial disclosures.
Figures
Similar articles
-
Mortality and failure-to-rescue after esophagectomy in the procedure-targeted National Surgical Quality Improvement Program registry.World J Surg. 2024 Sep;48(9):2235-2242. doi: 10.1002/wjs.12297. Epub 2024 Jul 23. World J Surg. 2024. PMID: 39044328
-
Morbidity of colectomy during pancreatoduodenectomy: An analysis of the pancreas-targeted American College of Surgeons National Surgical Quality Improvement Program Registry.J Hepatobiliary Pancreat Sci. 2023 May;30(5):655-663. doi: 10.1002/jhbp.1259. Epub 2022 Nov 11. J Hepatobiliary Pancreat Sci. 2023. PMID: 36282586
-
Factors influencing failure to rescue after pancreaticoduodenectomy: a National Surgical Quality Improvement Project Perspective.J Surg Res. 2017 Jun 15;214:131-139. doi: 10.1016/j.jss.2016.09.005. Epub 2016 Sep 8. J Surg Res. 2017. PMID: 28624034
-
Pancreatic resection in Veterans Affairs and selected university medical centers: results of the patient safety in surgery study.J Am Coll Surg. 2007 Jun;204(6):1252-60. doi: 10.1016/j.jamcollsurg.2007.03.015. J Am Coll Surg. 2007. PMID: 17544083
-
Variation in the definition of 'failure to rescue' from postoperative complications: a systematic review and recommendations for outcome reporting.Surgery. 2024 Apr;175(4):1103-1110. doi: 10.1016/j.surg.2023.12.006. Epub 2024 Jan 19. Surgery. 2024. PMID: 38245447
Cited by
-
Rescue from complications after pancreaticoduodenectomies at a low-volume Caribbean center: Value of tailored peri-pancreatectomy protocols.World J Gastrointest Surg. 2024 Mar 27;16(3):681-688. doi: 10.4240/wjgs.v16.i3.681. World J Gastrointest Surg. 2024. PMID: 38577074 Free PMC article.
-
Pancreaticoduodenectomies with Concurrent Colectomies: Indications, Technical Issues, Complications, and Oncological Outcomes.J Clin Med. 2023 Dec 14;12(24):7682. doi: 10.3390/jcm12247682. J Clin Med. 2023. PMID: 38137749 Free PMC article. Review.
-
The role of national population-based registries in pancreatic cancer surgery research.Int J Surg. 2024 Oct 1;110(10):6155-6162. doi: 10.1097/JS9.0000000000001405. Int J Surg. 2024. PMID: 38573130 Free PMC article. Review.
References
-
- Soden PA, Zettervall SL, Ultee KH, et al. Patient selection and perioperative outcomes are similar between targeted and nontargeted hospitals (in the National Surgical Quality Improvement Program) for abdominal aortic aneurysm repair. J Vasc Surg. Feb 2017;65(2):362–371. doi:10.1016/j.jvs.2016.04.066 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
