

Persistent symptoms after COVID-19 are not associated with differential SARS-CoV-2 antibody or T cell immunity
- PMID: 37612310
- PMCID: PMC10447583
- DOI: 10.1038/s41467-023-40460-1
Persistent symptoms after COVID-19 are not associated with differential SARS-CoV-2 antibody or T cell immunity
Abstract
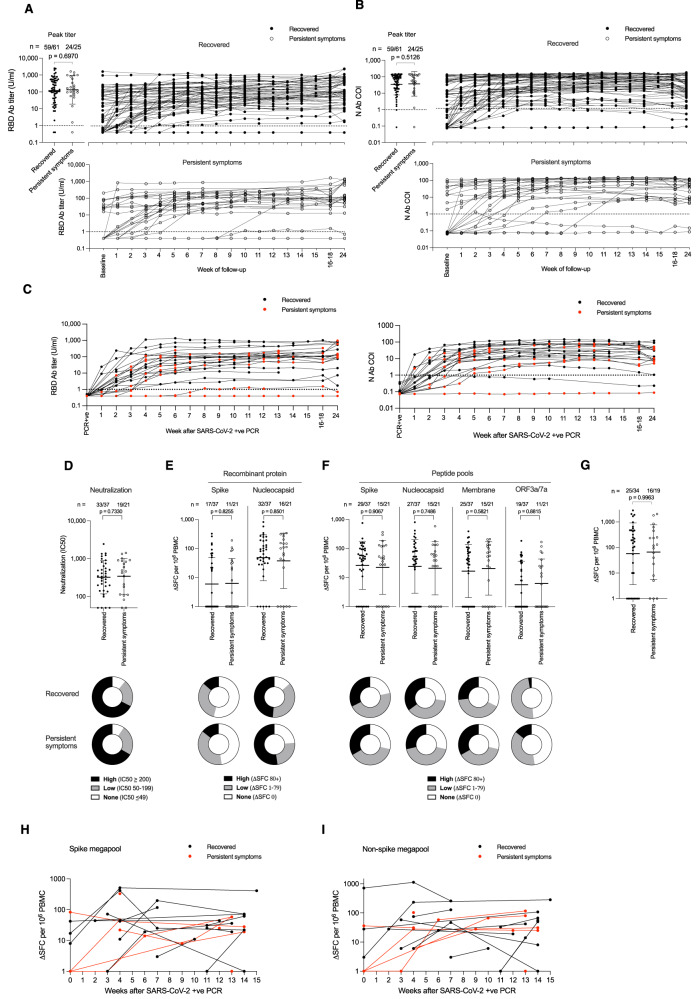
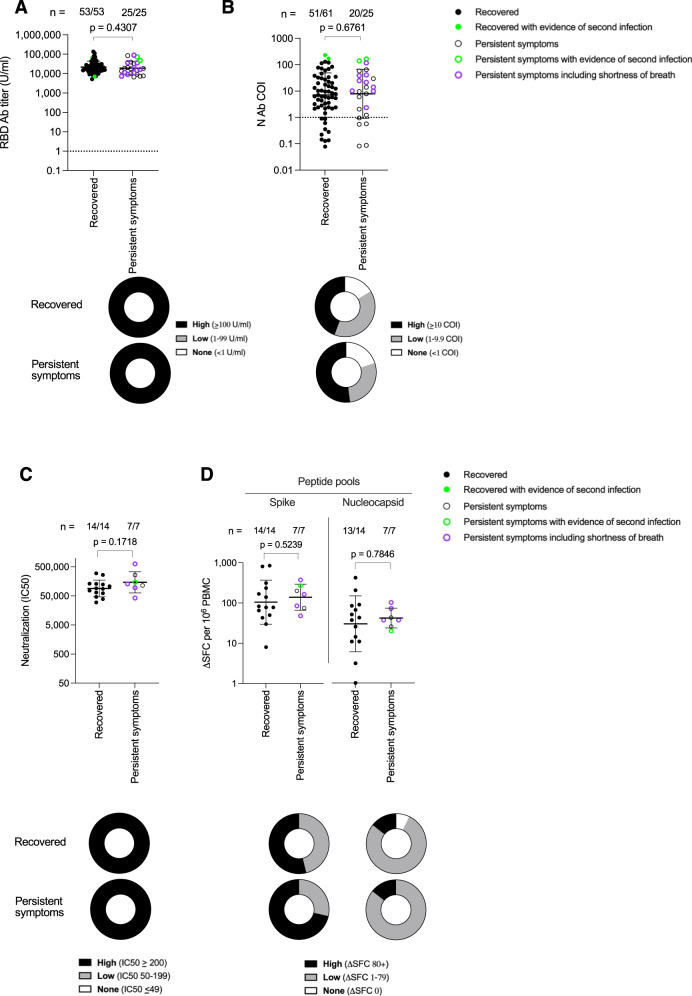
Among the unknowns in decoding the pathogenesis of SARS-CoV-2 persistent symptoms in Long Covid is whether there is a contributory role of abnormal immunity during acute infection. It has been proposed that Long Covid is a consequence of either an excessive or inadequate initial immune response. Here, we analyze SARS-CoV-2 humoral and cellular immunity in 86 healthcare workers with laboratory confirmed mild or asymptomatic SARS-CoV-2 infection during the first wave. Symptom questionnaires allow stratification into those with persistent symptoms and those without for comparison. During the period up to 18-weeks post-infection, we observe no difference in antibody responses to spike RBD or nucleoprotein, virus neutralization, or T cell responses. Also, there is no difference in the profile of antibody waning. Analysis at 1-year, after two vaccine doses, comparing those with persistent symptoms to those without, again shows similar SARS-CoV-2 immunity. Thus, quantitative differences in these measured parameters of SARS-CoV-2 adaptive immunity following mild or asymptomatic acute infection are unlikely to have contributed to Long Covid causality. ClinicalTrials.gov (NCT04318314).
© 2023. Springer Nature Limited.
Conflict of interest statement
R.J.B. and D.M.A. are members of the Global T cell Expert Consortium and have consulted for Oxford Immunotec outside the submitted work. DMA has received honorarium payments from Pfizer, AstraZeneca and Novavax for consultancy work. The remaining authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
