

A case of acquired hemophilia A after pancreaticoduodenectomy for distal cholangiocarcinoma
- PMID: 37614988
- PMCID: PMC10442756
- DOI: 10.3892/br.2023.1643
A case of acquired hemophilia A after pancreaticoduodenectomy for distal cholangiocarcinoma
Abstract
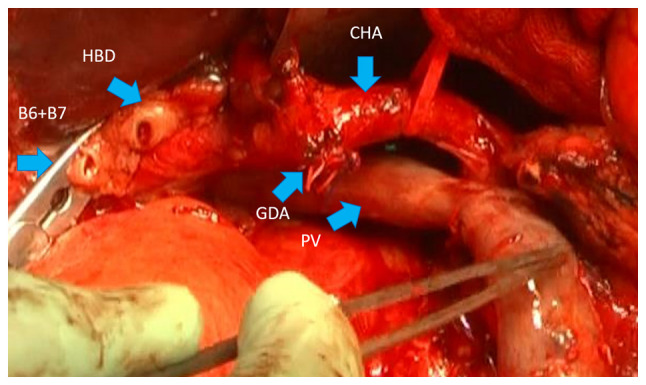
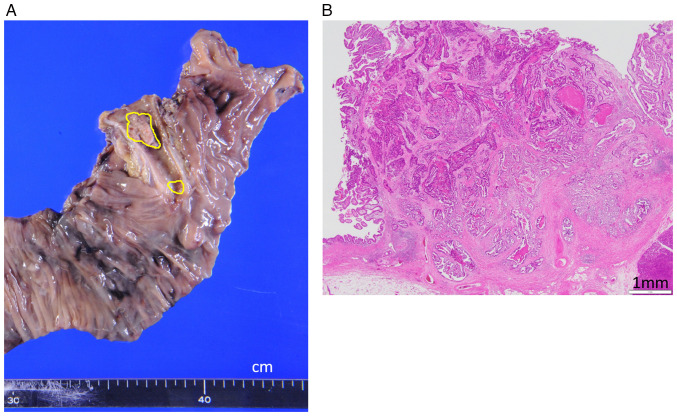
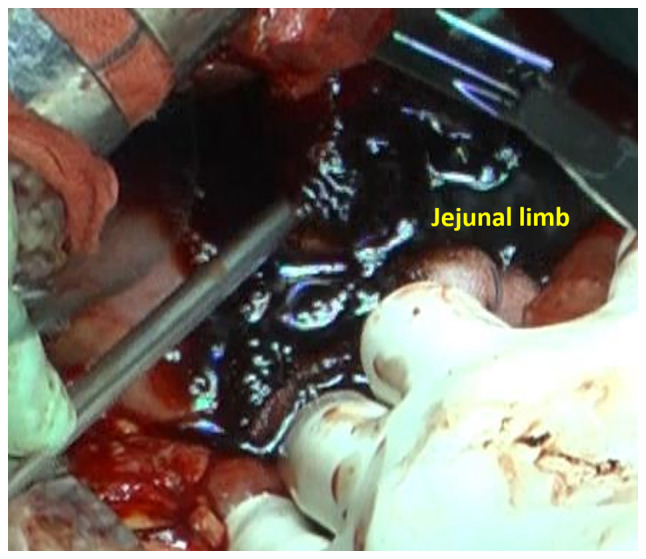
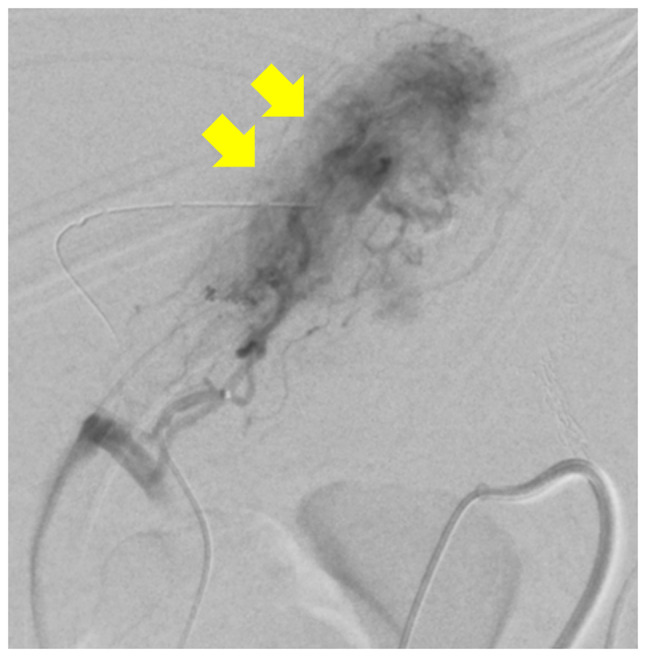
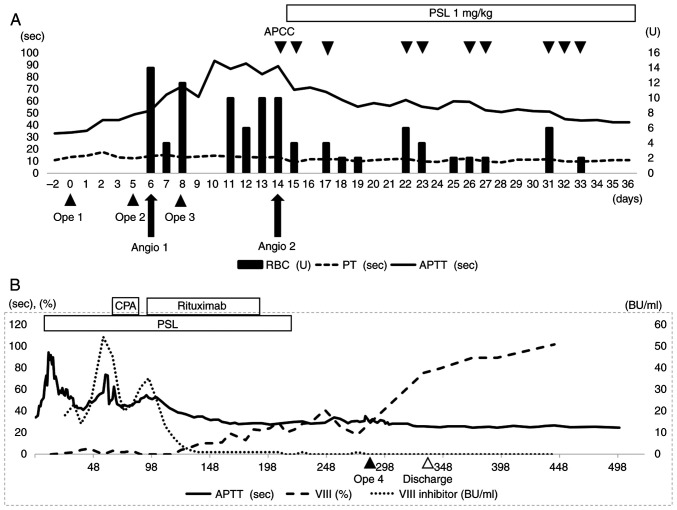
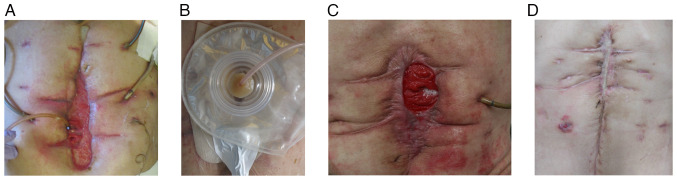
Acquired hemophilia A (AHA) is a rare disease that results from factor VIII inhibitors causing abnormal coagulation, and certain cases may develop after highly invasive surgery. The present case study reports on a 68-year-old male patient who developed AHA after undergoing a subtotal stomach-preserving pancreatoduodenectomy for distal cholangiocarcinoma. The patient experienced complications after surgery, requiring reoperation on postoperative day (PD) 5 due to rupture of the Braun's enterostomy. On PD 6, angiography was performed after bleeding was detected in the jejunal limb, but hemostasis occurred spontaneously during the examination. Bleeding was observed again on PD 8 and direct surgical ligation was performed. On PD 14, bleeding recurred in the jejunal limb and angiography was performed to embolize the periphery of the second jejunal artery. During the procedure, the prothrombin time was normal, but only the activated partial thromboplastin time was prolonged. A close examination of the coagulation system revealed a decrease in factor VIII levels and the presence of factor VIII inhibitors, resulting in the diagnosis of AHA. Administration of steroids was initiated on PD 15 and, in addition to daily blood transfusions, activated prothrombin complex concentrate was administered to achieve hemostasis. The patient was discharged from the intensive care unit on PD 36 but later developed an intractable labial fistula due to suture failure at the gastrojejunostomy site. As the use of factor VIII inhibitors continued despite the administration of steroids, cyclophosphamide (CPA) pulse therapy was added at PD 58. However, CPA was ineffective and the administration of rituximab was initiated on PD 98. After 12 courses of rituximab, the patient tested negative for factor VIII inhibitors on PD 219. On PD 289, labial fistula closure was performed with continuous replacement of factor VIII and the patient was discharged on PD 342.
Keywords: acquired hemophilia A; activated prothrombin complex concentrate; distal cholangiocarcinoma; factor VIII inhibitor; recombinant factor VIII preparation; rituximab; subtotal stomach-preserving pancreaticoduodenectomy; surgery.
Copyright: © Takahashi et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Acquired hemophilia A developing in the perioperative period of pancreatoduodenectomy: a report of two cases.Surg Case Rep. 2023 May 10;9(1):75. doi: 10.1186/s40792-023-01656-1. Surg Case Rep. 2023. PMID: 37162596 Free PMC article.
-
Acquired hemophilia in the patient suffering from rheumatoid arthritis: case report.Blood Coagul Fibrinolysis. 2013 Dec;24(8):874-80. doi: 10.1097/MBC.0b013e3283646635. Blood Coagul Fibrinolysis. 2013. PMID: 24042266
-
Acquired hemophilia A that required surgical hemostasis of hematomas occupying oral cavity: a case report.J Med Case Rep. 2021 Feb 15;15(1):66. doi: 10.1186/s13256-021-02669-w. J Med Case Rep. 2021. PMID: 33583426 Free PMC article.
-
[Acquired hemophilia caused by autoantibodies against factor VIII coagulation activity. Clinical, biological study and therapeutic indications. Experience based on a study of 9 cases].Ann Med Interne (Paris). 1997;148(7):477-90. Ann Med Interne (Paris). 1997. PMID: 9538386 Review. French.
-
Acquired hemophilia a: diagnosis, aetiology, clinical spectrum and treatment options.Autoimmun Rev. 2011 Apr;10(6):311-6. doi: 10.1016/j.autrev.2010.11.005. Epub 2010 Nov 27. Autoimmun Rev. 2011. PMID: 21115138 Review.
References
-
- Ogawa Y, Amano K, Matsuo-Tezuka Y, Okada N, Murakami Y, Nakamura T, Yamaguchi-Suita H, Nogami K. ORIHIME study: Real-world treatment patterns and clinical outcomes of 338 patients with acquired hemophilia A from a Japanese administrative database. Int J Hematol. 2023;117:44–55. doi: 10.1007/s12185-022-03467-w. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials