

Risk factors for migraine disease progression: a narrative review for a patient-centered approach
- PMID: 37615752
- PMCID: PMC10632231
- DOI: 10.1007/s00415-023-11880-2
Risk factors for migraine disease progression: a narrative review for a patient-centered approach
Abstract
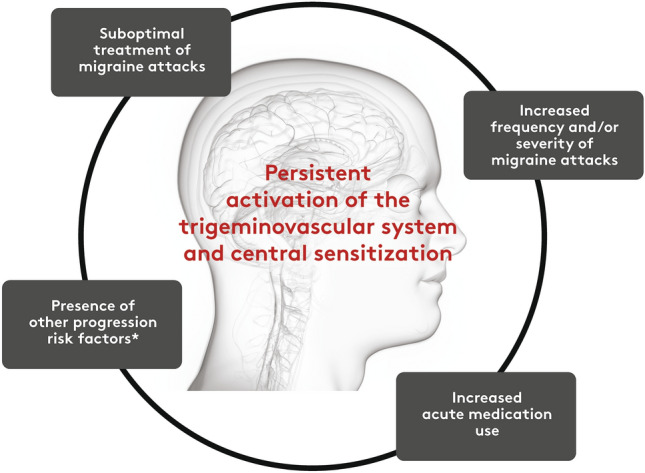
Background: In individuals with migraine, attacks may increase in frequency, severity, or both. Preventing migraine progression has emerged as a treatment goal in headache subspecialty practice, but there may be less awareness in general neurology or primary care settings where most people with migraine who seek treatment consult. Herein, we review the definition of and risk factors for migraine progression and consider strategies that could reduce its risk.
Methods: A group of headache expert healthcare professionals, clinicians, and researchers reviewed published evidence documenting factors associated with increased or decreased rates of migraine progression and established expert opinions for disease management recommendations. Strength of evidence was rated as good, moderate, or based solely on expert opinion, using modified criteria for causation developed by AB Hill.
Results: Migraine progression is commonly operationally defined as the transition from ≤ 15 to ≥ 15 monthly headache days among people with migraine; however, this does not necessarily constitute a fundamental change in migraine biology and other definitions should be considered. Established and theoretical key risk factors for migraine progression were categorized into five domains: migraine disease characteristics, treatment-related factors, comorbidities, lifestyle/exogenous factors, and demographic factors. Within these domains, good evidence supports the following risk factors: poorly optimized acute headache treatment, cutaneous allodynia, acute medication overuse, selected psychiatric symptoms, extra-cephalic chronic pain conditions, metabolism-related comorbidities, sleep disturbances, respiratory conditions, former/current high caffeine intake, physical inactivity, financial constraints, tobacco use, and personal triggers as risk factors. Protective actions that may mitigate migraine progression are sparsely investigated in published literature; our discussion of these factors is primarily based on expert opinion.
Conclusions: Recognizing risk factors for migraine progression will allow healthcare providers to suggest protective actions against migraine progression (Supplementary Fig. 1). Intervention studies are needed to weight the risk factors and test the clinical benefit of hypothesized mitigation strategies that emerge from epidemiological evidence.
Keywords: Chronic migraine; Episodic migraine; Migraine progression; Prevention strategies; Risk factors.
© 2023. The Author(s).
Conflict of interest statement
Dr. Lipton has been a consultant, advisory board member, and/or has received honoraria from Allergan/AbbVie, American Academy of Neurology, American Headache Society, Amgen, BioDelivery Sciences, Biohaven Pharmaceuticals, BioVision, electroCore, Eli Lilly, GlaxoSmithKline, Impel, Lundbeck Seattle BioPharmaceuticals, Merck, Pernix, Pfizer, Supernus, Teva, Trigemina, Vector, and Vedanta; has stock or stock options in Biohaven Pharmaceuticals and Manistee; and has received research support from Amgen, the FDA, the National Headache Foundation, and the NIH. Dr. Buse has received grant support from Amgen, the FDA, and the National Headache Foundation; has served as a consultant and received honoraria from Allergan/AbbVie, Amgen/Novartis, Biohaven, Collegium, Eli Lilly, Lundbeck, and Teva; and has served on the editorial board of
Figures
References
-
- Blumenfeld AM, Varon SF, Wilcox TK, Buse DC, Kawata AK, Manack A, Goadsby PJ, Lipton RB. Disability, HRQoL and resource use among chronic and episodic migraineurs: results from the International Burden of Migraine Study (IBMS) Cephalalgia. 2011;31:301–315. doi: 10.1177/0333102410381145. - DOI - PubMed
-
- Buse DC, Reed ML, Fanning KM, Bostic RC, Lipton RB. Demographics, headache features, and comorbidity profiles in relation to headache frequency in people with migraine: results of the American Migraine Prevalence and Prevention (AMPP) Study. Headache. 2020;60:2340–2356. doi: 10.1111/head.13966. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
