

Rare Variants in Complement Gene in C3 Glomerulopathy and Immunoglobulin-Mediated Membranoproliferative GN
- PMID: 37615951
- PMCID: PMC10637453
- DOI: 10.2215/CJN.0000000000000252
Rare Variants in Complement Gene in C3 Glomerulopathy and Immunoglobulin-Mediated Membranoproliferative GN
Abstract
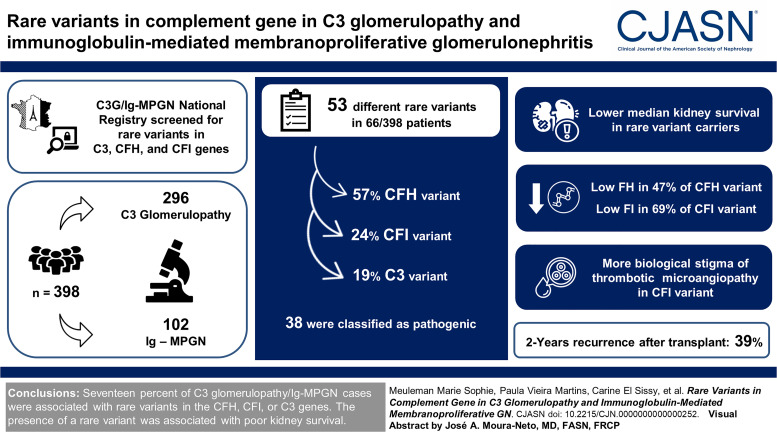
Background: C3 glomerulopathy and idiopathic immunoglobulin-mediated membranoproliferative GN (Ig-MPGN) are rare complement-mediated kidney diseases. Inherited forms of C3 glomerulopathy/Ig-MPGN are rarely described.
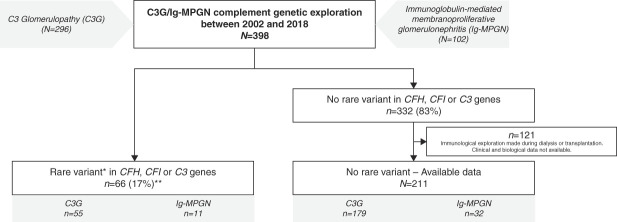
Methods: Three hundred ninety-eight patients with C3 glomerulopathy ( n =296) or Ig-MPGN ( n =102) from a national registry were screened for three complement genes: factor H ( CFH ), factor I ( CFI ), and C3 . Patients with rare variant (minor allele frequency <0.1%) were included. Epidemiologic, clinical, and immunologic data at diagnosis and kidney outcomes of patients were retrospectively collected.
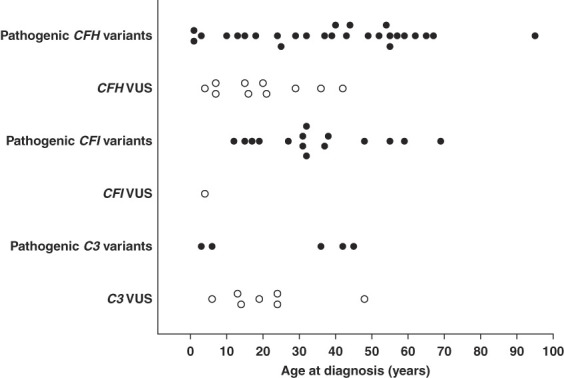
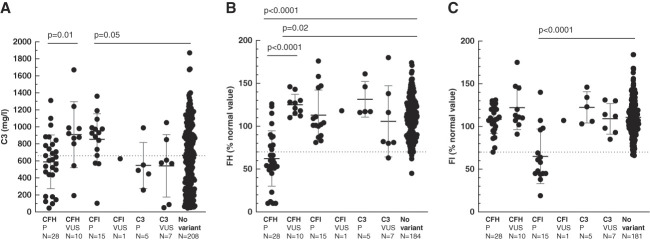
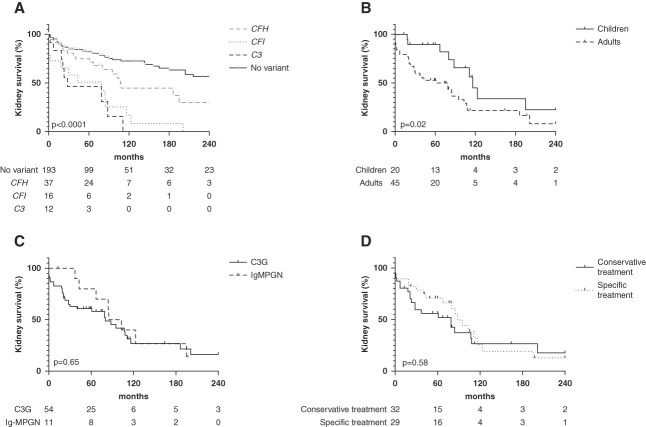
Results: Fifty-three different rare variants, including 30 (57%), 13 (24%), and ten (19%) in CFH , CFI , and C3 variants, were identified in 66/398 (17%) patients. Thirty-eight (72%) variants were classified as pathogenic, including 20/30 (66%) and 11/13 (84%) variants in CFH and CFI , respectively, impairing synthesis of factor H or factor I regulators. Fifteen of 53 (27%) variants were of unknown significance. At diagnosis, 69% of patients were adult (median age of 31 years). With the exception of biologic stigma of thrombotic microangiopathy, which was more frequent in patients with CFI variants (5/14 [36%] versus 1/37 [3%] and 0% in the CFH group and C3 group, respectively, P < 0.001), the clinical and histologic features were similar among the three variants groups. The kidney outcome was poor regardless of the age at onset and treatment received. Sixty-five percent (43/66) of patients with rare variant reach kidney failure after a median delay of 41 (19-104) months, compared with 28% (55/195) after a median delay of 34 (12-143) months in the nonvariant group. Among 36 patients who received a kidney transplant, 2-year recurrence was frequent, occurring in 39% (12/31), without difference between variant groups, and led to graft failure in three cases.
Conclusions: In our cohort, 17% of C3 glomerulopathy/Ig-MPGN cases were associated with rare variants in the CFH , CFI , or C3 genes. In most cases, a quantitative deficiency in factor H or factor I was identified. The presence of a rare variant was associated with poor kidney survival.
Podcast: This article contains a podcast at https://dts.podtrac.com/redirect.mp3/www.asn-online.org/media/podcast/CJASN/2023_11_08_CJN0000000000000252.mp3.
Copyright © 2023 by the American Society of Nephrology.
Conflict of interest statement
V. Audard reports consultancy for Advisory boards of Addmledica, Alnylam, AstraZeneca, Bayer, and Vifor pharma; honoraria for Advisory boards for Addmledica, Alnylam, AstraZeneca, Bayer, and Vifor pharma; and advisory or leadership roles on Advisory boards for Addmledica, Alnylam, AstraZeneca, Bayer, and Vifor pharma. F. Bridoux reports research funding from Baxter and Janssen; honoraria from AstraZeneca, Janssen, and Sanofi; advisory or leadership roles for AstraZeneca, Attralus, Janssen, Novartis, and Prothena; and speakers bureau for AstraZeneca, Janssen, and Sanofi. V. Esnault reports consultancy from Alexion, AstraZeneca, Bayer, BMS-Pfizer, Boehringer-Ingelheim, and Novartis; research funding from AstraZeneca, BMS-Pfizer, Boehringer-Ingelheim, Hemotech, and Novartis; honoraria from Alexion, Amgen, Bayer, BMS-Pfizer, Boehringer-Ingelheim, Fresenius, Lilly, and Novartis; and advisory or leadership roles for AstraZeneca, Bayer, and Boehringer-Ingelheim. V. Frémeaux-Bacchi served as consultant for Alexion Pharmaceuticals, Apellis, BioCryps, Novartis, Roche, Sobi, and UCB; reports research funding from Alexion Pharmaceuticals; honoraria from Alexion Pharmaceuticals, Apellis, BioCryps, Novartis, Roche, Sobi, and UCB; and advisory or leadership roles for Alexion Pharmaceuticals, Apellis, BioCryps, Novartis, and Sobi. N. Jourde-Chiche reports consultancy for Alexion, GSK, Otsuka, and Vifor and role as a Otsuka advisory board member (paid) and Vifor advisory board member (paid). A. Karras reports consultancy for Alnylam, GSK, Novartis, Otsuka, and Vifor; honoraria from AstraZeneca, Bohringer-Ingelheim, GSK, Novartis, Otsuka, Pfizer, and Vifor; advisory or leadership role for Novartis, Otsuka, and Vifor; and speakers bureau for AstraZeneca, Boehringer-Ingelheim, Otsuka, Pfizer, and Vifor. M. Le Quintrec reports consultancy for Alexion, GSK, Novartis, and Sanofi; research funding from Alexion and Sanofi; honoraria from Alexion, Astellas, GSK, Novartis, and Sanofi; and advisory or leadership role for Novartis French board. F. Provot reports consultancy from Alexion, Astellas, and Sanofi and advisory or leadership roles for Novartis, Sanofi, and Takeda. P. Remy reports honoraria from Biogen and BMS. A. Servais reports consultancy for Chiesi; honoraria from Alexion, Chiesi, Recordati, and Vertex; and advisory or leadership role for Novartis. E. Thervet reports consultancy for Pfizer and Vifor; research funding from Alexion and GSK; and honoraria from Pfizer and Vifor. J. Zuber reports consultancy for Alexion Pharma and honoraria from Alexion Pharmaceuticals and BMS Pharmaceuticals. All remaining authors have nothing to disclose.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
