

Predictors of outcomes in mild pulmonary hypertension according to 2022 ESC/ERS Guidelines: the EVIDENCE-PAH UK study
- PMID: 37619574
- PMCID: PMC10659956
- DOI: 10.1093/eurheartj/ehad532
Predictors of outcomes in mild pulmonary hypertension according to 2022 ESC/ERS Guidelines: the EVIDENCE-PAH UK study
Abstract
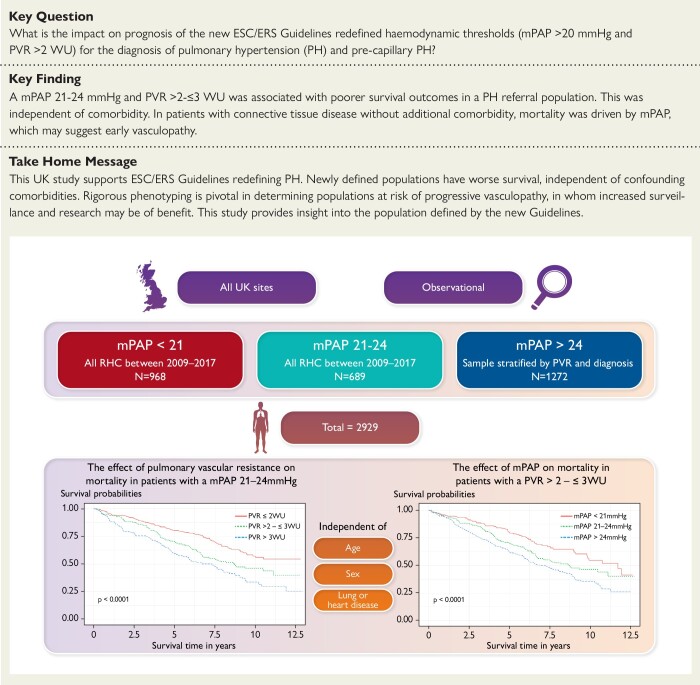
Background and aims: Interventional studies in pulmonary arterial hypertension completed to date have shown to be effective in symptomatic patients with significantly elevated mean pulmonary artery pressure (mPAP) (≥25 mmHg) and pulmonary vascular resistance (PVR) > 3 Wood Unit (WU). However, in health the mPAP does not exceed 20 mmHg and PVR is 2 WU or lower, at rest. The ESC/ERS guidelines have recently been updated to reflect this. There is limited published data on the nature of these newly defined populations (mPAP 21-24 mmHg and PVR >2-≤3 WU) and the role of comorbidity in determining their natural history. With the change in guidelines, there is a need to understand this population and the impact of the ESC/ERS guidelines in greater detail.
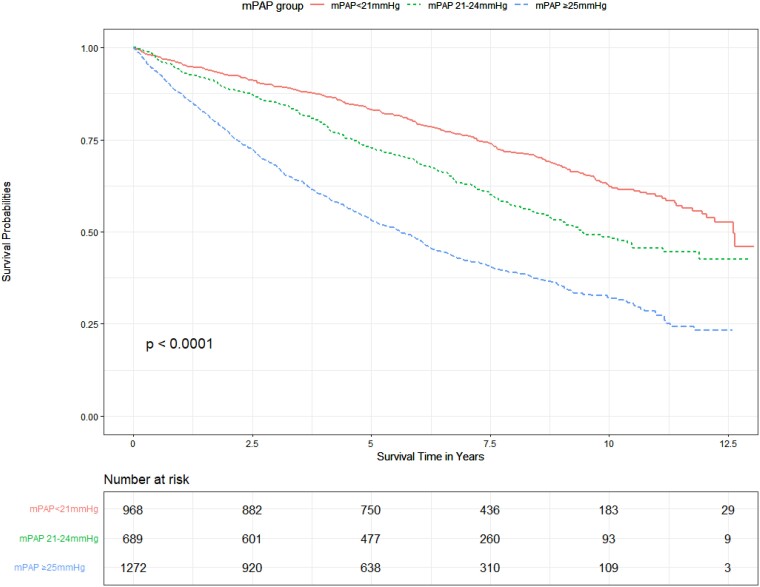
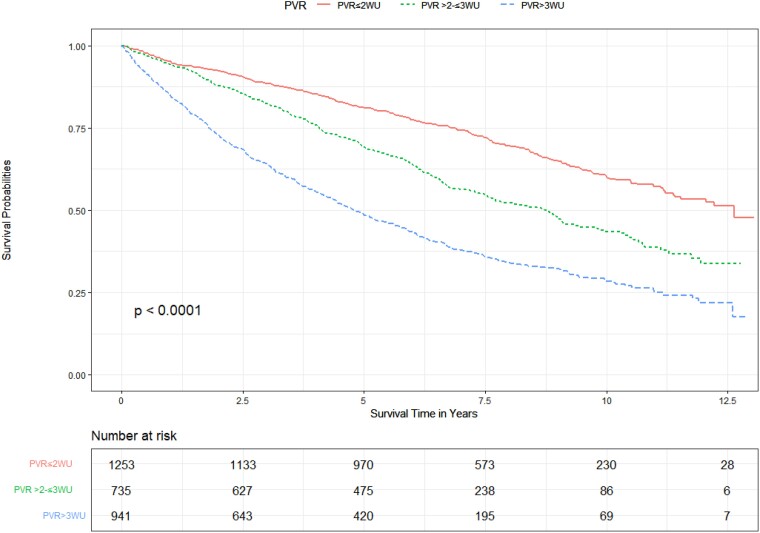
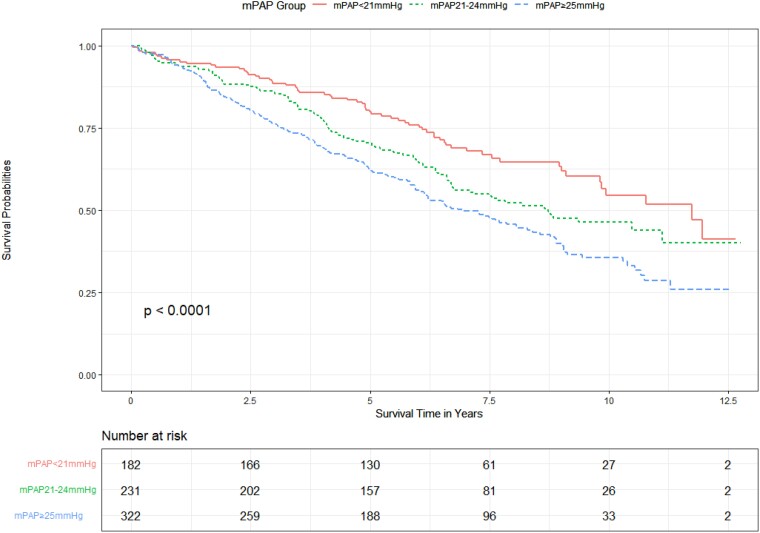
Methods: A retrospective nationwide evaluation of the role of pulmonary haemodynamics and comorbidity in predicting survival among patients referred to the UK pulmonary hypertension (PH) centres between 2009 and 2017. In total, 2929 patients were included in the study. Patients were stratified by mPAP (<21 mmHg, 21-24 mmHg, and ≥25 mmHg) and PVR (≤2 WU, > 2-≤3 WU, and >3 WU), with 968 (33.0%) in the mPAP <21 mmHg group, 689 (23.5%) in the mPAP 21-24 mmHg group, and 1272 (43.4%) in the mPAP ≥25 mmHg group.
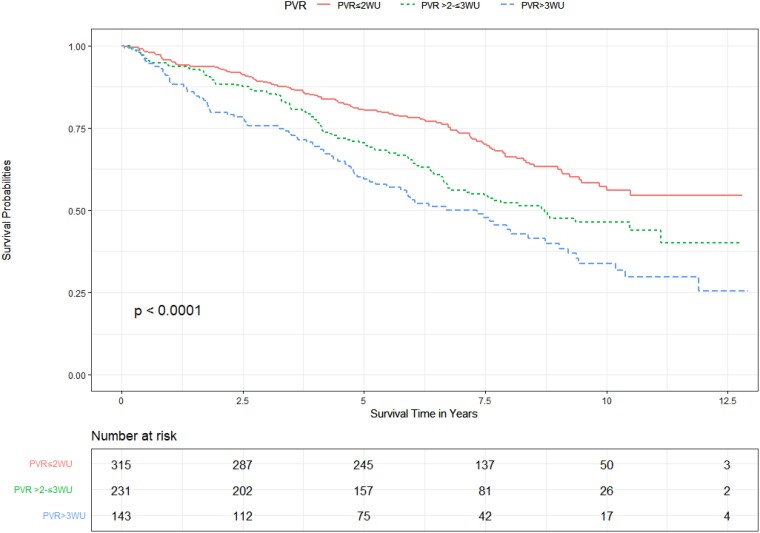
Results: Survival was negatively correlated with mPAP and PVR in the population as a whole. Survival in patients with mildly elevated mPAP (21-24 mmHg) or PVR (>2-≤3WU) was lower than among those with normal pressures (mPAP <21 mmHg) and normal PVR (PVR ≤ 2WU) independent of comorbid lung and heart disease [hazard ratio (HR) 1.36, 95% confidence interval (CI) 1.14-1.61, P = .0004 for mPAP vs. HR 1.28, 95% CI 1.10-1.49, P = .0012 for PVR]. Among patients with mildly elevated mPAP, a mildly elevated PVR remained an independent predictor of survival when adjusted for comorbid lung and heart disease (HR 1.33, 95% CI 1.01-1.75, P = .042 vs. HR 1.4, 95% CI 1.06-1.86, P = .019). 68.2% of patients with a mPAP 21-24 mmHg had evidence of underlying heart or lung disease. Patients with mildly abnormal haemodynamics were not more symptomatic than patients with normal haemodynamics. Excluding patients with heart and lung disease, connective tissue disease was associated with a poorer survival among those with PH. In this subpopulation evaluating those with a mPAP of 21-24 mmHg, survival curves only diverged after 5 years.
Conclusions: This study supports the change in diagnostic category of the ESC/ERS guidelines in a PH population. The newly included patients have an increased mortality independent of significant lung or heart disease. The majority of patients in this new category have underlying heart or lung disease rather than an isolated pulmonary vasculopathy. Mortality is higher if comorbidity is present. Rigorous phenotyping will be pivotal to determine which patients are at risk of progressive vasculopathic disease and in whom surveillance and recruitment to studies may be of benefit. This study provides an insight into the population defined by the new guidelines.
Keywords: Comorbidity; Haemodynamics; Mean pulmonary artery pressure; Pulmonary hypertension.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Confirmation of survival prediction based on 2022 ESC/ERS pulmonary hypertension guidelines new haemodynamic thresholds.Eur Heart J. 2023 Nov 21;44(44):4692-4695. doi: 10.1093/eurheartj/ehad672. Eur Heart J. 2023. PMID: 37944164 No abstract available.
Comment on
-
Confirmation of survival prediction based on 2022 ESC/ERS pulmonary hypertension guidelines new haemodynamic thresholds.Eur Heart J. 2023 Nov 21;44(44):4692-4695. doi: 10.1093/eurheartj/ehad672. Eur Heart J. 2023. PMID: 37944164 No abstract available.
References
-
- World Health Organization . Primary Pulmonary Hypertension. Geneva: Report on WHO Meeting; 1975.
-
- Galie N, Humbert M, Vachiery JL, Gibbs S, Lang I, Torbicki A, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Heart J 2016;37:67–119. 10.1093/eurheartj/ehv317 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
