

Diurnal rhythms of wrist temperature are associated with future disease risk in the UK Biobank
- PMID: 37620332
- PMCID: PMC10449859
- DOI: 10.1038/s41467-023-40977-5
Diurnal rhythms of wrist temperature are associated with future disease risk in the UK Biobank
Abstract
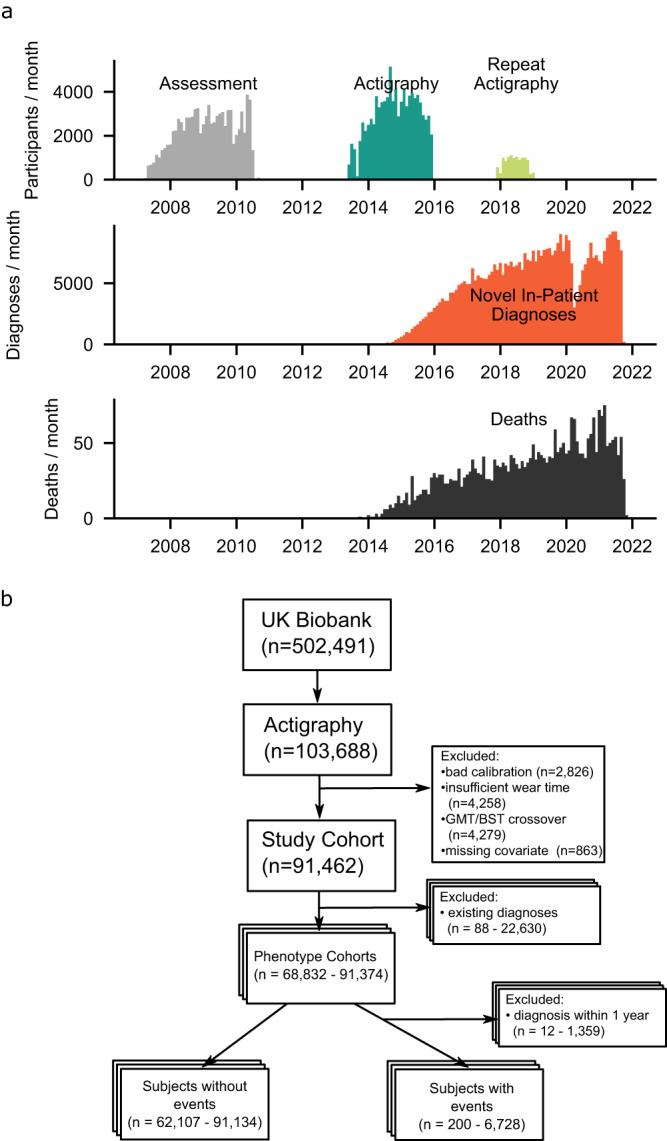
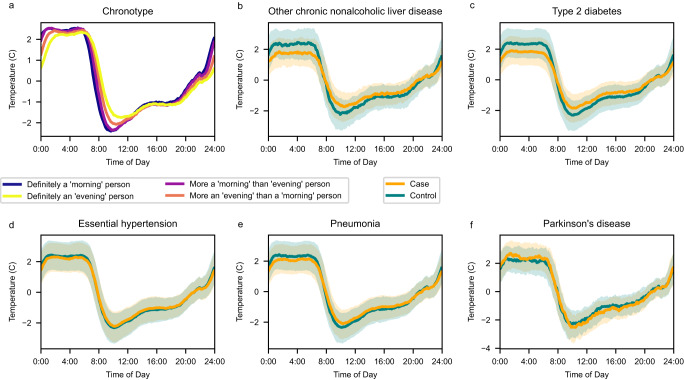
Many chronic disease symptomatologies involve desynchronized sleep-wake cycles, indicative of disrupted biorhythms. This can be interrogated using body temperature rhythms, which have circadian as well as sleep-wake behavior/environmental evoked components. Here, we investigated the association of wrist temperature amplitudes with a future onset of disease in the UK Biobank one year after actigraphy. Among 425 disease conditions (range n = 200-6728) compared to controls (range n = 62,107-91,134), a total of 73 (17%) disease phenotypes were significantly associated with decreased amplitudes of wrist temperature (Benjamini-Hochberg FDR q < 0.05) and 26 (6.1%) PheCODEs passed a more stringent significance level (Bonferroni-correction α < 0.05). A two-standard deviation (1.8° Celsius) lower wrist temperature amplitude corresponded to hazard ratios of 1.91 (1.58-2.31 95% CI) for NAFLD, 1.69 (1.53-1.88) for type 2 diabetes, 1.25 (1.14-1.37) for renal failure, 1.23 (1.17-1.3) for hypertension, and 1.22 (1.11-1.33) for pneumonia (phenome-wide atlas available at http://bioinf.itmat.upenn.edu/biorhythm_atlas/ ). This work suggests peripheral thermoregulation as a digital biomarker.
© 2023. Springer Nature Limited.
Conflict of interest statement
G.A.F. is an advisor to Calico Laboratories. T.G.B. received funding from Calico Laboratories. C.S. is an advisor to Antibe Therapeutics Inc and received funding from Calico Laboratories. The authors declare no other competing interests.
Figures


Update of
-
Diurnal rhythmicity of wearable device-measured wrist temperature predicts future disease incidence in the UK Biobank.Res Sq [Preprint]. 2023 Feb 15:rs.3.rs-2535978. doi: 10.21203/rs.3.rs-2535978/v1. Res Sq. 2023. Update in: Nat Commun. 2023 Aug 24;14(1):5172. doi: 10.1038/s41467-023-40977-5. PMID: 36824952 Free PMC article. Updated. Preprint.
References
-
- Benefits of Physical Activity. Centers for Disease Control and Prevention, https://www.cdc.gov/physicalactivity/basics/pa-health/index.htm (2022).
-
- Basics About Sleep. Centers for Disease Control and Prevention, https://www.cdc.gov/sleep/about_sleep/index.html (2022).
-
- (No authors listed) Fitbit step counts clarify the association between activity and chronic disease risk. Nat. Med.28, 2263–2264 (2022). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
