

Effect of semaglutide on major adverse cardiovascular events by baseline kidney parameters in participants with type 2 diabetes and at high risk of cardiovascular disease: SUSTAIN 6 and PIONEER 6 post hoc pooled analysis
- PMID: 37620807
- PMCID: PMC10463803
- DOI: 10.1186/s12933-023-01949-7
Effect of semaglutide on major adverse cardiovascular events by baseline kidney parameters in participants with type 2 diabetes and at high risk of cardiovascular disease: SUSTAIN 6 and PIONEER 6 post hoc pooled analysis
Abstract
Background: Semaglutide is a glucose-lowering treatment for type 2 diabetes (T2D) with demonstrated cardiovascular benefits; semaglutide may also have kidney-protective effects. This post hoc analysis investigated the association between major adverse cardiovascular events (MACE) and baseline kidney parameters and whether the effect of semaglutide on MACE risk was impacted by baseline kidney parameters in people with T2D at high cardiovascular risk.
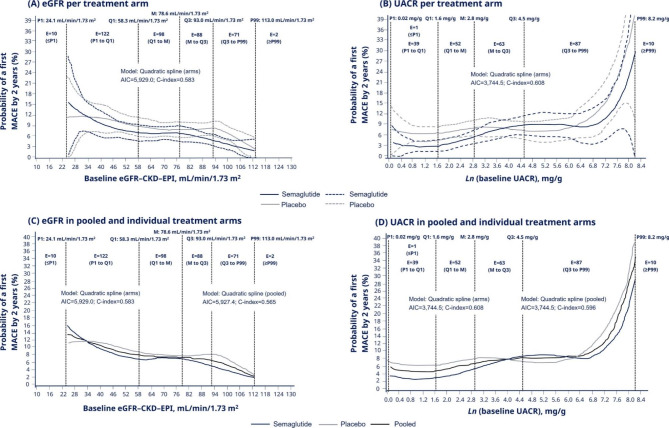
Methods: Participants from the SUSTAIN 6 and PIONEER 6 trials, receiving semaglutide or placebo, were categorised according to baseline kidney function (estimated glomerular filtration rate [eGFR] < 45 and ≥ 45-<60 versus ≥ 60 mL/min/1.73 m2) or damage (urine albumin:creatinine ratio [UACR] ≥ 30-≤300 and > 300 versus < 30 mg/g). Relative risk of first MACE by baseline kidney parameters was evaluated using a Cox proportional hazards model. The same model, adjusted with inverse probability weighting, and a quadratic spline regression were applied to evaluate the effect of semaglutide on risk and event rate of first MACE across subgroups. The semaglutide effects on glycated haemoglobin (HbA1c), body weight (BW) and serious adverse events (SAEs) across subgroups were also evaluated.
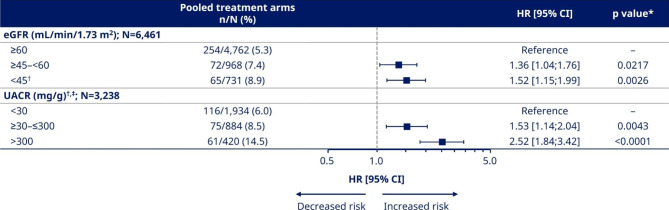
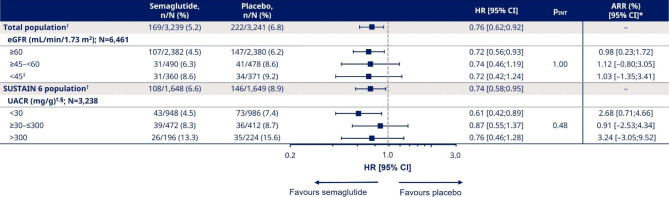
Results: Independently of treatment, participants with reduced kidney function (eGFR ≥ 45-<60 and < 45 mL/min/1.73 m2: hazard ratio [95% confidence interval]; 1.36 [1.04;1.76] and 1.52 [1.15;1.99]) and increased albuminuria (UACR ≥ 30-≤300 and > 300 mg/g: 1.53 [1.14;2.04] and 2.52 [1.84;3.42]) had an increased MACE risk versus those without. Semaglutide consistently reduced MACE risk versus placebo across all eGFR and UACR subgroups (interaction p value [pINT] > 0.05). Semaglutide reduced HbA1c regardless of baseline eGFR and UACR (pINT>0.05); reductions in BW were affected by baseline eGFR (pINT<0.001) but not UACR (pINT>0.05). More participants in the lower eGFR or higher UACR subgroups experienced SAEs versus participants in reference groups; the number of SAEs was similar between semaglutide and placebo arms in each subgroup.
Conclusions: MACE risk was greater for participants with kidney impairment or damage than for those without. Semaglutide consistently reduced MACE risk across eGFR and UACR subgroups, indicating that semaglutide provides cardiovascular benefits in people with T2D and at high cardiovascular risk across a broad spectrum of kidney function and damage.
Trial registrations: NCT01720446; NCT02692716.
Keywords: Cardiovascular disease; Estimated glomerular filtration rate; Glucagon-like peptide-1 receptor agonist; Kidney disease; Major cardiovascular events; NCT01720446; NCT02692716; Semaglutide; Type 2 diabetes; Urine albumin:creatinine ratio.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
PR received grants from AstraZeneca, Bayer, Novo Nordisk A/S, as well as consulting fees from AstraZeneca, Astellas, Bayer, Boehringer Ingelheim, Gilead, Merck, Mundipharma, Novo Nordisk A/S and Sanofi. SCB received grants, teaching sponsorship and honoraria from AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Eli Lilly, GlaxoSmithKline, Merck Sharp & Dohme, Novo Nordisk A/S, Pfizer, Sanofi and Takeda. HBT, ES and SR are employees of Novo Nordisk A/S, Denmark; HBT and SR also own stocks or stock options in Novo Nordisk A/S. HJLH received grants from AstraZeneca, Bayer, Boehringer Ingelheim, Janssen and Novo Nordisk A/S; consulting fees from AstraZeneca, Bayer, Boehringer Ingelheim, Chinook, CSL Behring, Dimerix, Eli Lilly, Fresenius, Gilead, Janssen, Novo Nordisk A/S, Novartis and Travere Therapeutics; honoraria from AstraZeneca and Novo Nordisk A/S; travel and/or other support for attending meetings from AstraZeneca and Eli Lilly. LGM received grants, honoraria and consulting fees for advisory boards from Novo Nordisk A/S.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
