

Pneumocystis jirovecii pneumonia in intensive care units: a multicenter study by ESGCIP and EFISG
- PMID: 37620828
- PMCID: PMC10464114
- DOI: 10.1186/s13054-023-04608-1
Pneumocystis jirovecii pneumonia in intensive care units: a multicenter study by ESGCIP and EFISG
Abstract
Background: Pneumocystis jirovecii pneumonia (PJP) is an opportunistic, life-threatening disease commonly affecting immunocompromised patients. The distribution of predisposing diseases or conditions in critically ill patients admitted to intensive care unit (ICU) and subjected to diagnostic work-up for PJP has seldom been explored.
Materials and methods: The primary objective of the study was to describe the characteristics of ICU patients subjected to diagnostic workup for PJP. The secondary objectives were: (i) to assess demographic and clinical variables associated with PJP; (ii) to assess the performance of Pneumocystis PCR on respiratory specimens and serum BDG for the diagnosis of PJP; (iii) to describe 30-day and 90-day mortality in the study population.
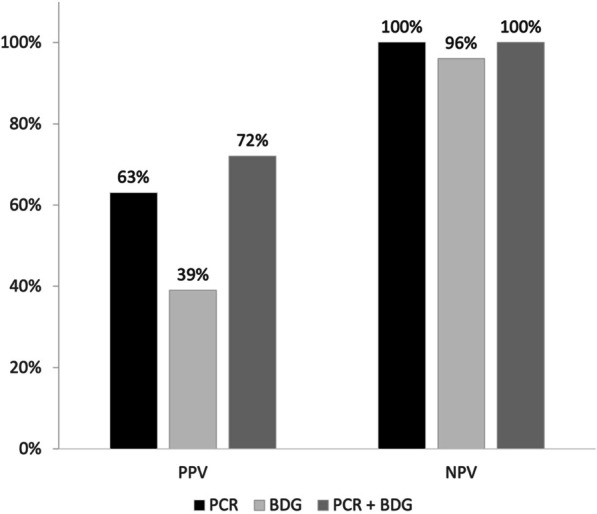
Results: Overall, 600 patients were included in the study, of whom 115 had presumptive/proven PJP (19.2%). Only 8.8% of ICU patients subjected to diagnostic workup for PJP had HIV infection, whereas hematological malignancy, solid tumor, inflammatory diseases, and solid organ transplants were present in 23.2%, 16.2%, 15.5%, and 10.0% of tested patients, respectively. In multivariable analysis, AIDS (odds ratio [OR] 3.31; 95% confidence interval [CI] 1.13-9.64, p = 0.029), non-Hodgkin lymphoma (OR 3.71; 95% CI 1.23-11.18, p = 0.020), vasculitis (OR 5.95; 95% CI 1.07-33.22, p = 0.042), metastatic solid tumor (OR 4.31; 95% CI 1.76-10.53, p = 0.001), and bilateral ground glass on CT scan (OR 2.19; 95% CI 1.01-4.78, p = 0.048) were associated with PJP, whereas an inverse association was observed for increasing lymphocyte cell count (OR 0.64; 95% CI 0.42-1.00, p = 0.049). For the diagnosis of PJP, higher positive predictive value (PPV) was observed when both respiratory Pneumocystis PCR and serum BDG were positive compared to individual assay positivity (72% for the combination vs. 63% for PCR and 39% for BDG). Cumulative 30-day mortality and 90-day mortality in patients with presumptive/proven PJP were 52% and 67%, respectively.
Conclusion: PJP in critically ill patients admitted to ICU is nowadays most encountered in non-HIV patients. Serum BDG when used in combination with respiratory Pneumocystis PCR could help improve the certainty of PJP diagnosis.
Keywords: Biomarker; Diagnosis; ICU; PCR; Pneumocystis; Pneumonia; Serum β-D-Glucan.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
Outside the submitted work, DRG reports investigator-initiated grants from Pfizer, Shionogi, and Gilead Italia, and speaker and/or advisor fees from Pfizer and Tillotts Pharma. Outside the submitted work, MB reports research grants and/or personal fees for advisor/consultant and/or speaker/chairman from BioMérieux, Cidara, Gilead, Menarini, MSD, Pfizer, and Shionogi. Outside the submitted work, VDP reports research grant from Seegene Inc. Outside the submitted work, PLW performed diagnostic evaluations and received meeting sponsorship from Bruker; speakers fees, expert advice fees and meeting sponsorship from Gilead; expert advice fees from F2G and speaker fees from Pfizer; speakers fees and performed diagnostic evaluations for Associates of Cape Cod and IMMY. JW received meeting speakers and travel fees and investigator-initiated grants from MSD, Gilead and Pfizer, outside the scope of this manuscript. Outside the submitted work, PK reports grants or contracts from German Federal Ministry of Research and Education (BMBF) B-FAST (Bundesweites Forschungsnetz Angewandte Surveillance und Testung) and NAPKON (Nationales Pandemie Kohorten Netz, German National Pandemic Cohort Network) of the Network University Medicine (NUM) and the State of North Rhine-Westphalia; Consulting fees Ambu GmbH, Gilead Sciences, Mundipharma Resarch Limited, Noxxon N.V. and Pfizer Pharma; Honoraria for lectures from Akademie für Infektionsmedizin e.V., Ambu GmbH, Astellas Pharma, BioRad Laboratories Inc., Datamed GmbH, European Confederation of Medical Mycology, Gilead Sciences, GPR Academy Ruesselsheim, HELIOS Kliniken GmbH, Lahn-Dill-Kliniken GmbH, medupdate GmbH, MedMedia GmbH, MSD Sharp & Dohme GmbH, Pfizer Pharma GmbH, Scilink Comunicación Científica SC and University Hospital and LMU Munich; Participation on an Advisory Board from Ambu GmbH, Gilead Sciences, Mundipharma Resarch Limited and Pfizer Pharma; A pending patent currently reviewed at the German Patent and Trade Mark Office (DE 10 2021 113 007.7); Other non-financial interests from Elsevier, Wiley and Taylor & Francis online. The other authors report no conflicts of interests related to this study.
Figures
References
-
- Ford N, Shubber Z, Meintjes G, Grinsztejn B, Eholie S, Mills EJ, Davies MA, Vitoria M, Penazzato M, Nsanzimana S, et al. Causes of hospital admission among people living with HIV worldwide: a systematic review and meta-analysis. Lancet HIV. 2015;2(10):e438–444. doi: 10.1016/S2352-3018(15)00137-X. - DOI - PubMed
-
- Schmidt JJ, Lueck C, Ziesing S, Stoll M, Haller H, Gottlieb J, Eder M, Welte T, Hoeper MM, Scherag A, et al. Clinical course, treatment and outcome of Pneumocystis pneumonia in immunocompromised adults: a retrospective analysis over 17 years. Crit Care. 2018;22(1):307. doi: 10.1186/s13054-018-2221-8. - DOI - PMC - PubMed
-
- Pagano L, Fianchi L, Mele L, Girmenia C, Offidani M, Ricci P, Mitra ME, Picardi M, Caramatti C, Piccaluga P, et al. Pneumocystis carinii pneumonia in patients with malignant haematological diseases: 10 years' experience of infection in GIMEMA centres. Br J Haematol. 2002;117(2):379–386. doi: 10.1046/j.1365-2141.2002.03419.x. - DOI - PubMed
-
- Enomoto T, Azuma A, Kohno A, Kaneko K, Saito H, Kametaka M, Usuki J, Gemma A, Kudoh S, Nakamura S. Differences in the clinical characteristics of Pneumocystis jirovecii pneumonia in immunocompromized patients with and without HIV infection. Respirology. 2010;15(1):126–131. doi: 10.1111/j.1440-1843.2009.01660.x. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
