

Hemodynamic forces from 4D flow magnetic resonance imaging predict left ventricular remodeling following cardiac resynchronization therapy
- PMID: 37620886
- PMCID: PMC10463519
- DOI: 10.1186/s12968-023-00955-8
Hemodynamic forces from 4D flow magnetic resonance imaging predict left ventricular remodeling following cardiac resynchronization therapy
Abstract
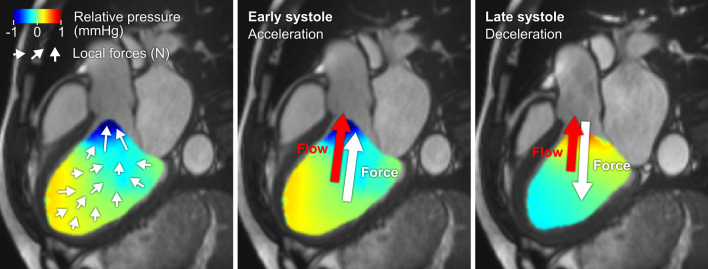
Background: Patients with heart failure and left bundle branch block (LBBB) may receive cardiac resynchronization therapy (CRT), but current selection criteria are imprecise, and many patients have limited treatment response. Hemodynamic forces (HDF) have been suggested as a marker for CRT response. The aim of this study was therefore to investigate left ventricular (LV) HDF as a predictive marker for LV remodeling after CRT.
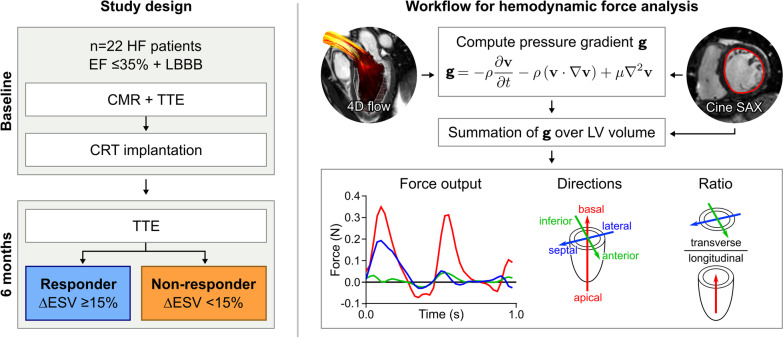
Methods: Patients with heart failure, EF < 35% and LBBB (n = 22) underwent CMR with 4D flow prior to CRT. LV HDF were computed in three directions using the Navier-Stokes equations, reported in median N [interquartile range], and the ratio of transverse/longitudinal HDF was calculated for systole and diastole. Transthoracic echocardiography was performed before and 6 months after CRT. Patients with end-systolic volume reduction ≥ 15% were defined as responders.
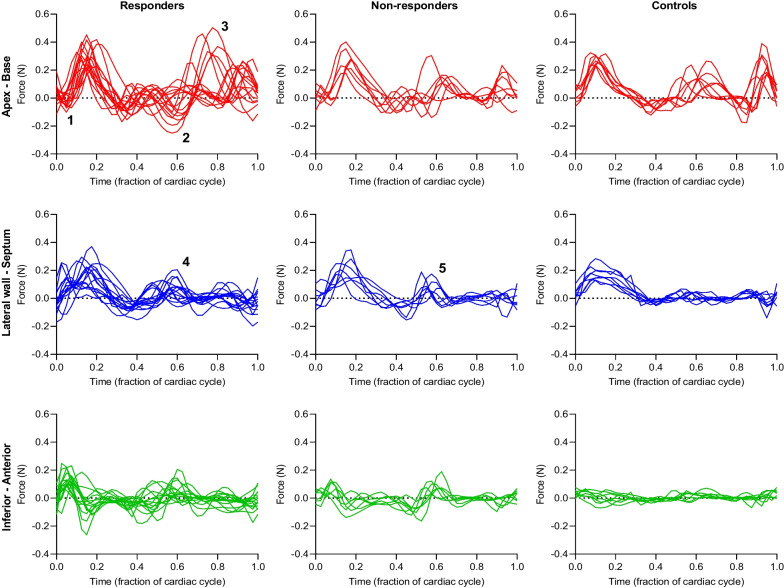
Results: Non-responders had smaller HDF than responders in the inferior-anterior direction in systole (0.06 [0.03] vs. 0.07 [0.03], p = 0.04), and in the apex-base direction in diastole (0.09 [0.02] vs. 0.1 [0.05], p = 0.047). Non-responders had larger diastolic HDF ratio compared to responders (0.89 vs. 0.67, p = 0.004). ROC analysis of diastolic HDF ratio for identifying CRT non-responders had AUC of 0.88 (p = 0.005) with sensitivity 57% and specificity 100% for ratio > 0.87. Intragroup comparison found higher HDF ratio in systole compared to diastole for responders (p = 0.003), but not for non-responders (p = 0.8).
Conclusion: Hemodynamic force ratio is a potential marker for identifying patients with heart failure and LBBB who are unlikely to benefit from CRT. Larger-scale studies are required before implementation of HDF analysis into clinical practice.
Keywords: Cardiac magnetic resonance; Device response; Heart failure with reduced ejection fraction; Left bundle branch block; Pacemaker.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
-
- Freemantle N, Tharmanathan P, Calvert MJ, Abraham WT, Ghosh J, Cleland JGF. Cardiac resynchronisation for patients with heart failure due to left ventricular systolic dysfunction—a systematic review and meta-analysis. Eur J Heart Fail. 2006;8(4):433–440. doi: 10.1016/j.ejheart.2005.11.014. - DOI - PubMed
-
- Pouleur A-C, Knappe D, Shah AM, Uno H, Bourgoun M, Foster E, et al. Relationship between improvement in left ventricular dyssynchrony and contractile function and clinical outcome with cardiac resynchronization therapy: the MADIT-CRT trial. Eur Heart J. 2011;32(14):1720–1729. doi: 10.1093/eurheartj/ehr185. - DOI - PubMed
-
- Solomon SD, Foster E, Bourgoun M, Shah A, Viloria E, Brown MW, et al. Effect of cardiac resynchronization therapy on reverse remodeling and relation to outcome: multicenter automatic defibrillator implantation trial: cardiac resynchronization therapy. Circulation. 2010;122(10):985–992. doi: 10.1161/CIRCULATIONAHA.110.955039. - DOI - PubMed
-
- Cleland JG, Abraham WT, Linde C, Gold MR, Young JB, Claude Daubert J, et al. An individual patient meta-analysis of five randomized trials assessing the effects of cardiac resynchronization therapy on morbidity and mortality in patients with symptomatic heart failure. Eur Heart J. 2013;34(46):3547–3556. doi: 10.1093/eurheartj/eht290. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
