

Comparison of Different Antibiotics and the Risk for Community-Associated Clostridioides difficile Infection: A Case-Control Study
- PMID: 37622034
- PMCID: PMC10444966
- DOI: 10.1093/ofid/ofad413
Comparison of Different Antibiotics and the Risk for Community-Associated Clostridioides difficile Infection: A Case-Control Study
Abstract
Background: Antibiotics are the greatest risk factor for Clostridioides difficile infection (CDI). Risk for CDI varies across antibiotic types and classes. Optimal prescribing and stewardship recommendations require comparisons of risk across antibiotics. However, many prior studies rely on aggregated antibiotic categories or are underpowered to detect significant differences across antibiotic types. Using a large database of real-world data, we evaluate community-associated CDI risk across individual antibiotic types.
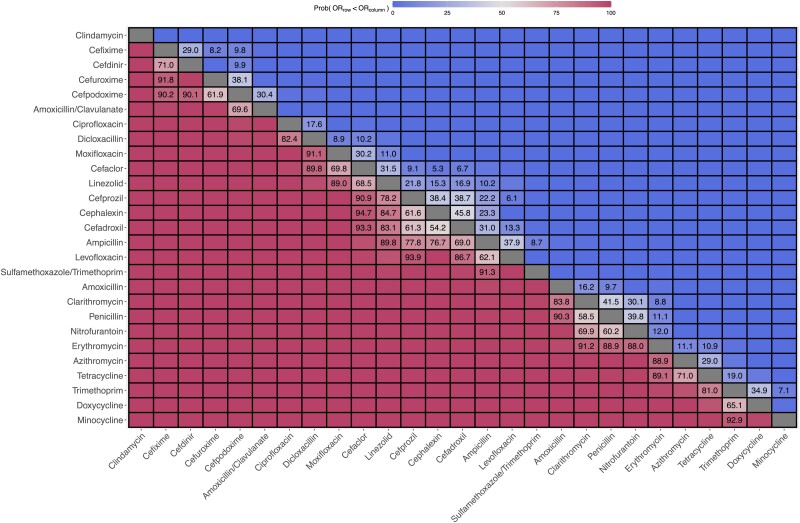
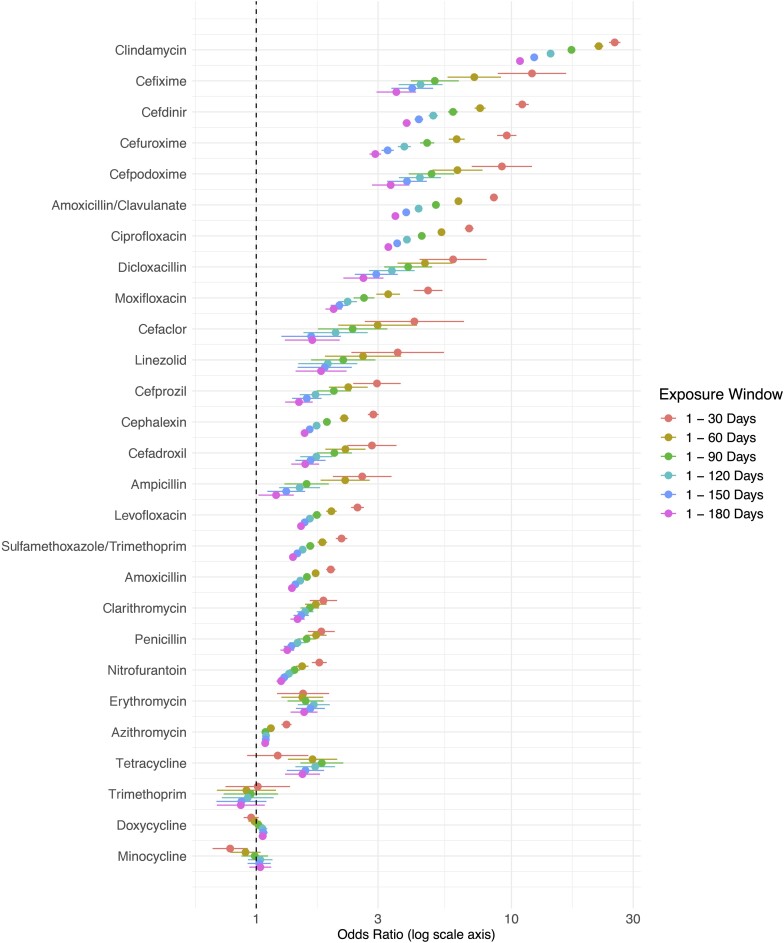
Methods: We conducted a matched case-control study using a large database of insurance claims capturing longitudinal health care encounters and medications. Case patients with community-associated CDI were matched to 5 control patients by age, sex, and enrollment period. Antibiotics prescribed within 30 days before the CDI diagnosis along with other risk factors, including comorbidities, health care exposures, and gastric acid suppression were considered. Conditional logistic regression and a Bayesian analysis were used to compare risk across individual antibiotics. A sensitivity analysis of antibiotic exposure windows between 30 and 180 days was conducted.
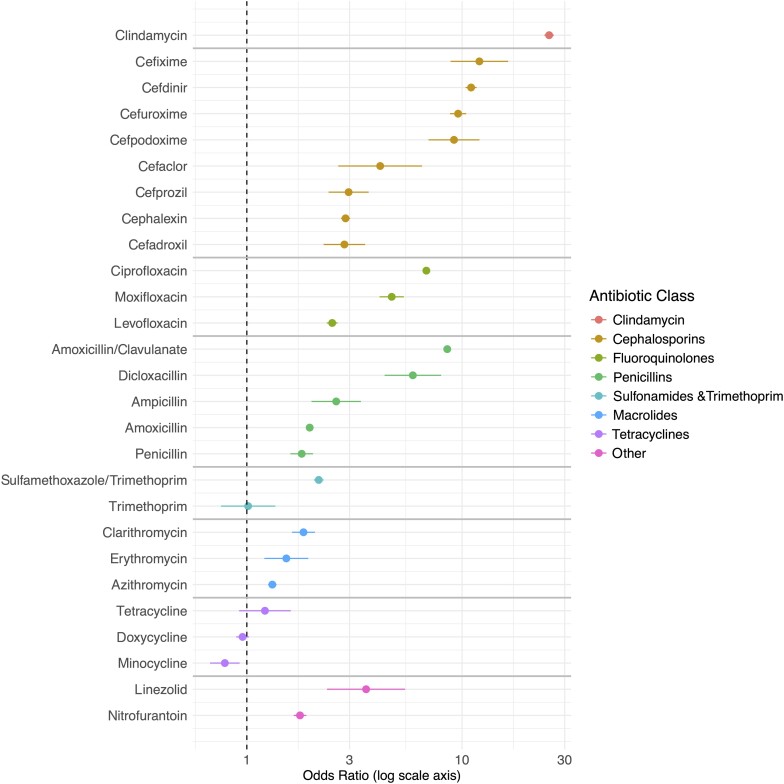
Results: We identified 159 404 cases and 797 020 controls. Antibiotics with the greatest risk for CDI included clindamycin and later-generation cephalosporins, and those with the lowest risk included minocycline and doxycycline. We were able to differentiate and order individual antibiotics in terms of their relative level of associated risk for CDI. Risk estimates varied considerably with different exposure windows considered.
Conclusions: We found wide variation in CDI risk within and between classes of antibiotics. These findings ordering the level of associated risk across antibiotics can help inform tradeoffs in antibiotic prescribing decisions and stewardship efforts.
Keywords: CDI; Clostridioides difficile infection; antibiotics; case–control study; outpatient; risk factors; stewardship.
© The Author(s) 2023. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. All authors: no reported conflicts.
Figures
Similar articles
-
Antibiotic Exposure and Risk for Hospital-Associated Clostridioides difficile Infection.Antimicrob Agents Chemother. 2020 Mar 24;64(4):e02169-19. doi: 10.1128/AAC.02169-19. Print 2020 Mar 24. Antimicrob Agents Chemother. 2020. PMID: 31964789 Free PMC article.
-
Antibiotic-Specific Risk for Community-Acquired Clostridioides difficile Infection in the United States from 2008 to 2020.Antimicrob Agents Chemother. 2022 Dec 20;66(12):e0112922. doi: 10.1128/aac.01129-22. Epub 2022 Nov 15. Antimicrob Agents Chemother. 2022. PMID: 36377887 Free PMC article.
-
Risk of Clostridioides difficile infection following different antibiotics: insights from multi-source medical data.Int J Antimicrob Agents. 2024 Oct;64(4):107288. doi: 10.1016/j.ijantimicag.2024.107288. Epub 2024 Jul 31. Int J Antimicrob Agents. 2024. PMID: 39089342
-
Antibiotics and healthcare facility-associated Clostridioides difficile infection: systematic review and meta-analysis 2020 update.J Antimicrob Chemother. 2021 Jun 18;76(7):1676-1688. doi: 10.1093/jac/dkab091. J Antimicrob Chemother. 2021. PMID: 33787887
-
Community-associated Clostridium difficile infection and antibiotics: a meta-analysis.J Antimicrob Chemother. 2013 Sep;68(9):1951-61. doi: 10.1093/jac/dkt129. Epub 2013 Apr 25. J Antimicrob Chemother. 2013. PMID: 23620467 Review.
Cited by
-
Proton-pump inhibitors increase C. difficile infection risk by altering pH rather than by affecting the gut microbiome based on a bioreactor model.Gut Microbes. 2025 Dec;17(1):2519697. doi: 10.1080/19490976.2025.2519697. Epub 2025 Jun 16. Gut Microbes. 2025. PMID: 40524314 Free PMC article.
-
The Impact of Human Milk Oligosaccharides on Antibiotic-Induced Microbial Dysbiosis and Gut Inflammation in Mice.Antibiotics (Basel). 2025 May 10;14(5):488. doi: 10.3390/antibiotics14050488. Antibiotics (Basel). 2025. PMID: 40426555 Free PMC article.
-
A Review of Therapies for Clostridioides difficile Infection.Antibiotics (Basel). 2024 Dec 31;14(1):17. doi: 10.3390/antibiotics14010017. Antibiotics (Basel). 2024. PMID: 39858303 Free PMC article. Review.
-
Approaching toxigenic Clostridia from a One Health perspective.Anaerobe. 2024 Jun;87:102839. doi: 10.1016/j.anaerobe.2024.102839. Epub 2024 Mar 27. Anaerobe. 2024. PMID: 38552896 Free PMC article. Review.
-
A Pharmacovigilance Study Regarding the Risk of Antibiotic-Associated Clostridioides difficile Infection Based on Reports from the EudraVigilance Database: Analysis of Some of the Most Used Antibiotics in Intensive Care Units.Pharmaceuticals (Basel). 2023 Nov 9;16(11):1585. doi: 10.3390/ph16111585. Pharmaceuticals (Basel). 2023. PMID: 38004450 Free PMC article.
References
-
- Kwon JH, Olsen MA, Dubberke ER. The morbidity, mortality, and costs associated with Clostridium difficile infection. Infect Dis Clin North Am 2015; 29:123–34. - PubMed
-
- Evans CT, Safdar N. Current trends in the epidemiology and outcomes of Clostridium difficile infection. Clin Infect Dis 2015; 60(Suppl 2):S66–71. - PubMed
