

Ischaemic stroke despite antiplatelet therapy: Causes and outcomes
- PMID: 37622482
- PMCID: PMC10472957
- DOI: 10.1177/23969873231174942
Ischaemic stroke despite antiplatelet therapy: Causes and outcomes
Abstract
Background: Ischaemic stroke may occur despite antiplatelet therapy (APT). We aimed to investigate frequency, potential causes and outcomes in patients with ischaemic stroke despite APT.
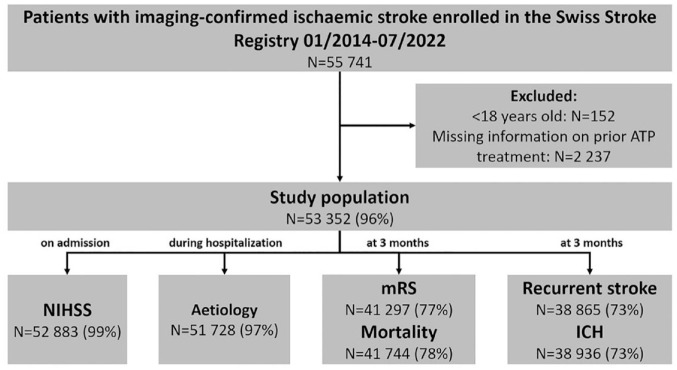
Methods: In this cohort study, we enrolled patients with imaging-confirmed ischaemic stroke from the Swiss Stroke Registry (01/2014-07/2022). We determined the frequency of prior APT, assessed stroke aetiology (modified TOAST classification) and determined the association of prior APT with unfavourable functional outcome (modified Rankin Scale score 3-6) and recurrent ischaemic stroke at 3 months using regression models.
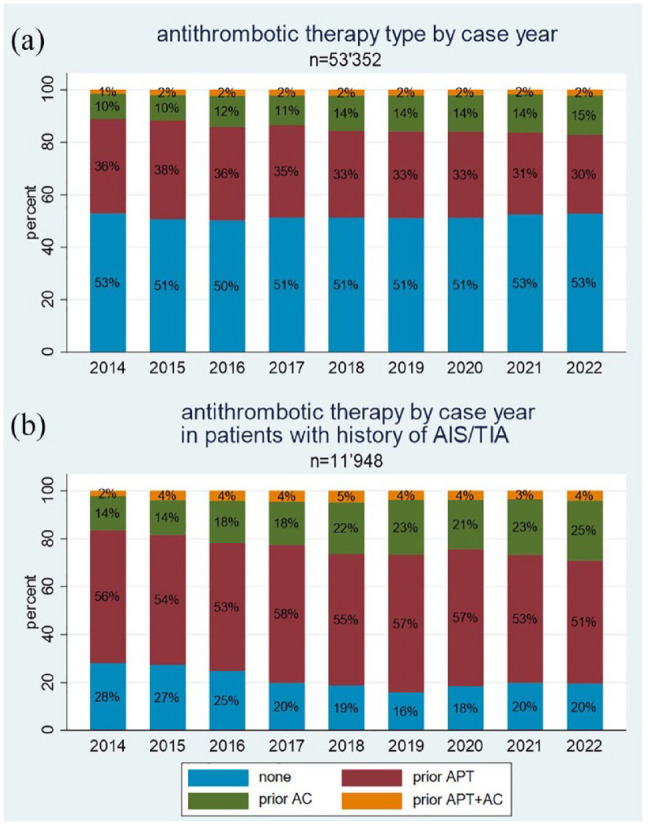
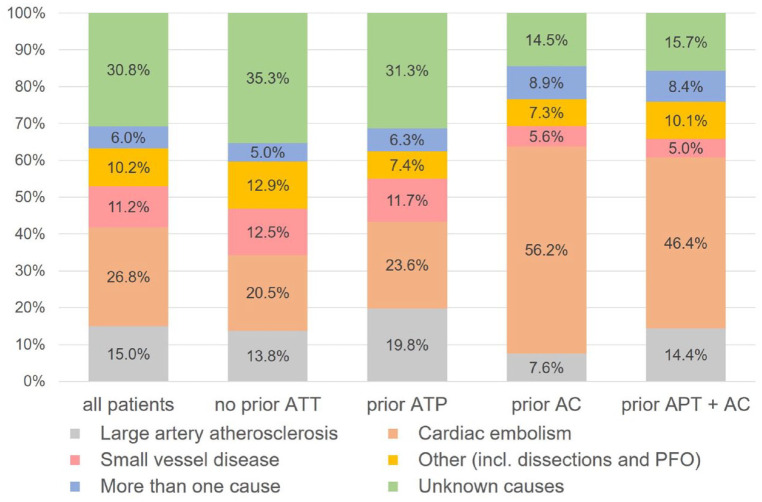
Results: Among 53,352 patients, 27,484 (51.5%) had no prior antithrombotic treatment, 17,760 (33.3%) were on APT, 7039 (13.2%) on anticoagulation and 1069 (2.0%) were on APT + anticoagulation. In patients with a history of ischaemic stroke/TIA (n = 11,948; 22.4%), 2401 (20.1%) had no prior antithrombotic therapy, 6594 (55.2%) were on APT, 2489 (20.8%) on anticoagulation and 464 (3.9%) on APT + anticoagulation. Amongst patients with ischaemic stroke despite APT, aetiology was large artery atherosclerosis in 19.8% (n = 3416), cardiac embolism in 23.6% (n = 4059), small vessel disease in 11.7% (n = 2011), other causes in 7.4% (n = 1267), more than one cause in 6.3% (n = 1078) and unknown cause in 31.3% (n = 5388). Prior APT was not independently associated with unfavourable outcome (aOR = 1.06; 95% CI: 0.98-1.14; p = 0.135) or death (aOR = 1.10; 95% CI: 0.99-1.21; p = 0.059) at 3-months but with increased odds of recurrent stroke (6.0% vs 4.3%; aOR 1.26; 95% CI: 1.11-1.44; p < 0.001).
Conclusions: One-third of ischaemic strokes occurred despite APT and 20% of patients with a history of ischaemic stroke had no antithrombotic therapy when having stroke recurrence. Aetiology of breakthrough strokes despite APT is heterogeneous and these patients are at increased risk of recurrent stroke.
Keywords: Acute ischaemic stroke; aetiology; anticoagulation; antiplatelet therapy; functional outcome; incidence; recurrent stroke; stroke severity.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AAT reported consultant and/or speaker fees from Mitsubishi Tanabe Pharma, Medtronic, AstraZeneca and Schwabe Pharma outside the submitted work. MK received research grants from the Swiss National Science Foundation (NR 182267; NR 204977; NR 198783), the Swiss Heart Foundation; the USZ-Foundation and has received nonfinancial support from B.R.A.H.M.S. Thermofisher Scientific as well as ROCHE Diagnostics, none related to this study. MK has served on the advisory board of Medtronic, Astra Zeneca, BMS/Pfizer and Bayer. MB reported consultant fees from Astra Zeneca and Sandoz outside the submitted work. TRM reported grants from Bangerter Rhyner Foundation, Swiss Heart Foundation and Swiss National Science Foundation outside the submitted work. DJS reported grants from Bangerter Rhyner Foundation and Swiss Heart Foundation outside the study; personal fees from Bayer, Alexion and VarmX outside the submitted work. No other disclosures/conflicts of interest were reported.
Figures
References
-
- Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2019; 50: e344–e418. - PubMed
-
- Xian Y, O’Brien EC, Liang L, et al. Association of preceding antithrombotic treatment with acute ischemic stroke severity and in-hospital outcomes among patients with atrial fibrillation. JAMA 2017; 317: 1057–1067. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
