

Pregnancy-specific alcohol policies and admissions to substance use disorder treatment for pregnant people in the USA
- PMID: 37623929
- PMCID: PMC10642603
- DOI: 10.1093/alcalc/agad056
Pregnancy-specific alcohol policies and admissions to substance use disorder treatment for pregnant people in the USA
Abstract
Aims: We examined relationships between pregnancy-specific alcohol policies and admissions to substance use disorder treatment for pregnant people in the USA.
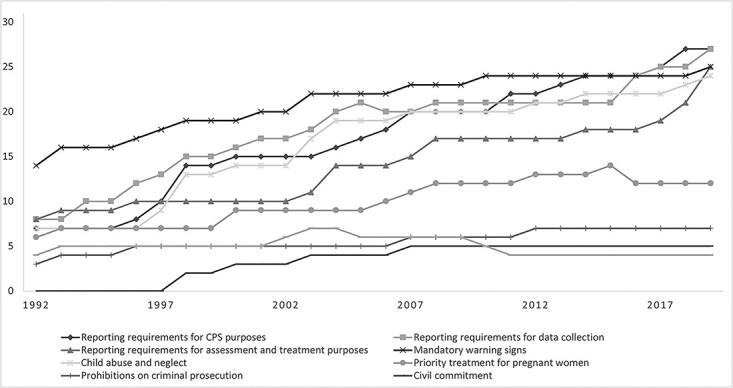
Methods: We merged state-level policy and treatment admissions data for 1992-2019. We aggregated data by state-year to examine effects of nine pregnancy-specific alcohol policies on the number of admissions of pregnant women where alcohol was reported as the primary, secondary, or tertiary substance related to the treatment episode (N = 1331). We fit Poisson models that included all policy variables, state-level controls, fixed effects for state and year, state-specific time trends, and an offset variable of the number of pregnancies in the state-year to account for differences in population size and fertility.
Results: When alcohol was reported as the primary substance, civil commitment [incidence rate ratio (IRR) 1.45, 95% CI: 1.10-1.89] and reporting requirements for assessment and treatment purposes [IRR 1.36, 95% CI: 1.04-1.77] were associated with greater treatment admissions. Findings for alcohol as primary, secondary, or tertiary substance were similar for civil commitment [IRR 1.31, 95% CI: 1.08-1.59] and reporting requirements for assessment and treatment purposes [IRR 1.21, 95% CI: 1.00-1.47], although mandatory warning signs [IRR 0.84, 95% CI: 0.72-0.98] and priority treatment for pregnant women [IRR 0.88, 95% CI: 0.78-0.99] were associated with fewer treatment admissions. Priority treatment findings were not robust in sensitivity analyses. No other policies were associated with treatment admissions.
Conclusions: Pregnancy-specific alcohol policies related to greater treatment admissions tend to mandate treatment rather than make voluntary treatment more accessible, raising questions of ethics and effectiveness.
Keywords: alcohol; policy; pregnancy.
© The Author(s) 2023. Medical Council on Alcohol and Oxford University Press. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- American Public Health Association . Public Health Code of Ethics. Washington, DC: American Public Health Association, 2019.
-
- Angelotta C, Weiss CJ, Angelotta JW. et al. A moral or medical problem? The relationship between legal penalties and treatment practices for opioid use disorders in pregnant women. Womens Health Issues 2016;26:595–601. - PubMed
-
- Atkins DN, Durrance CP. State policies that treat prenatal substance use as child abuse or neglect fail to achieve their intended goals. Health Aff (Millwood) 2020;39:756–63. - PubMed
-
- Centers for Disease Control and Prevention (CDC) . Alcohol consumption among pregnant and childbearing-aged women—United States, 1991 and 1995. MMWR Morb Mortal Wkly Rep 1997;46:346–50. - PubMed
