

The COVID-19 Pandemic and Associated Inequities in Acute Myocardial Infarction Treatment and Outcomes
- PMID: 37624599
- PMCID: PMC10457721
- DOI: 10.1001/jamanetworkopen.2023.30327
The COVID-19 Pandemic and Associated Inequities in Acute Myocardial Infarction Treatment and Outcomes
Abstract
Importance: The COVID-19 pandemic disrupted usual care for emergent conditions, such as acute myocardial infarction (AMI). Understanding whether Black and Hispanic individuals experiencing AMI had greater increases in poor outcomes compared with White individuals during the pandemic has important equity implications.
Objective: To investigate whether the COVID-19 pandemic was associated with increased disparities in treatment and outcomes among Medicare patients hospitalized with AMI.
Design, setting, and participants: This cross-sectional study used Medicare data for patients hospitalized with AMI between January 2016 and November 2020. Patients were categorized as Hispanic, non-Hispanic Black, and non-Hispanic White. The association between race and ethnicity and outcomes as a function of the proportion of hospitalized patients with COVID-19 was evaluated using interrupted time series. Data were analyzed from October 2022 to June 2023.
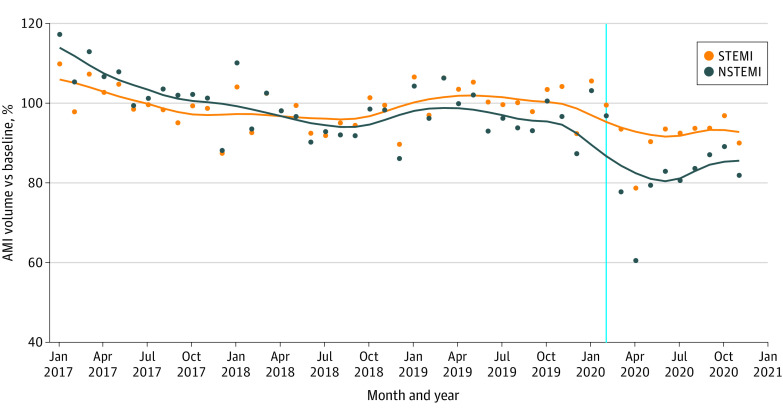
Exposure: The main exposure was a hospital's proportion of hospitalized patients with COVID-19 on a weekly basis as a proxy for care disruption during the pandemic.
Main outcomes and measures: Revascularization, 30-day mortality, 30-day readmission, and nonhome discharges.
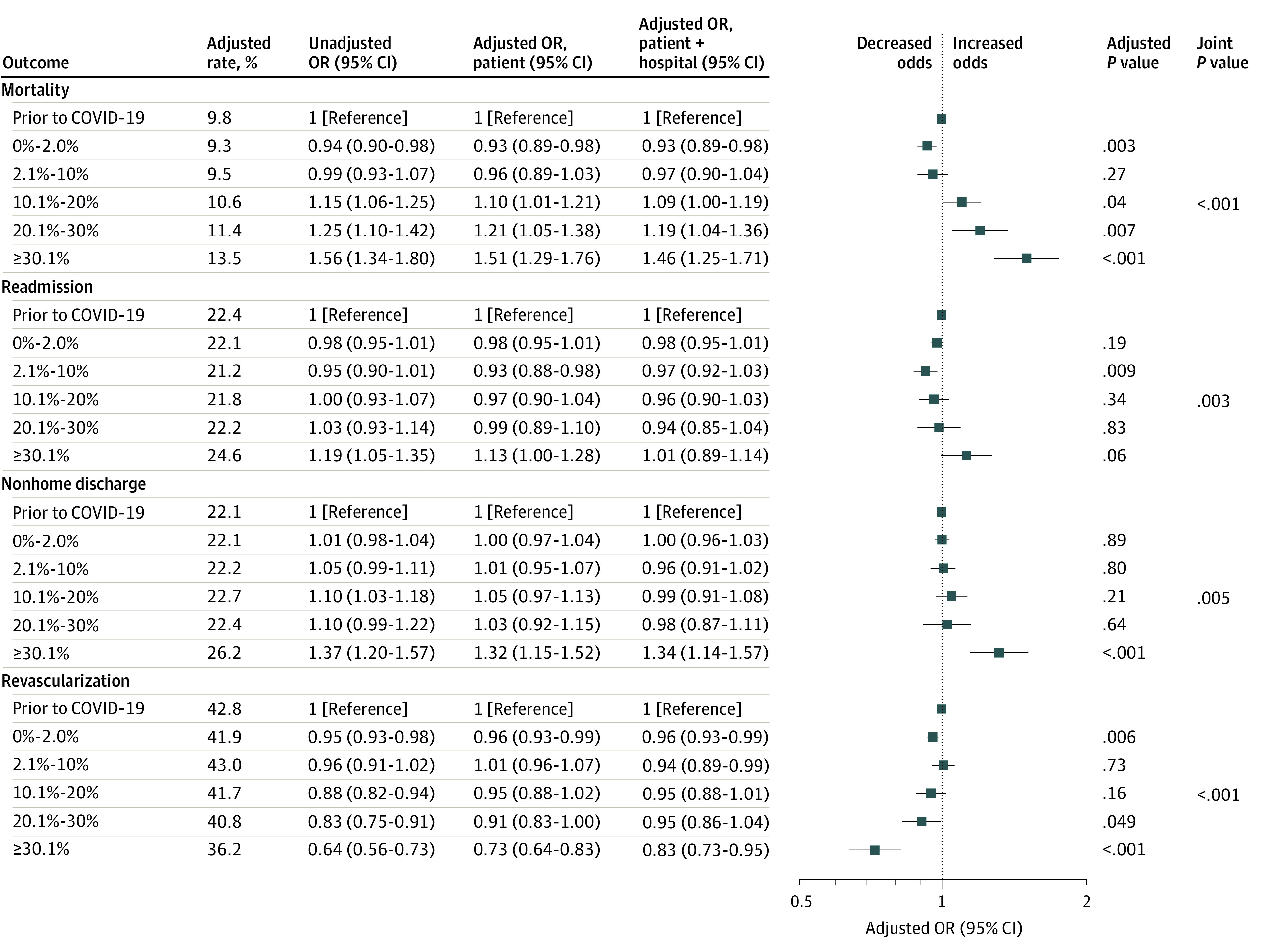
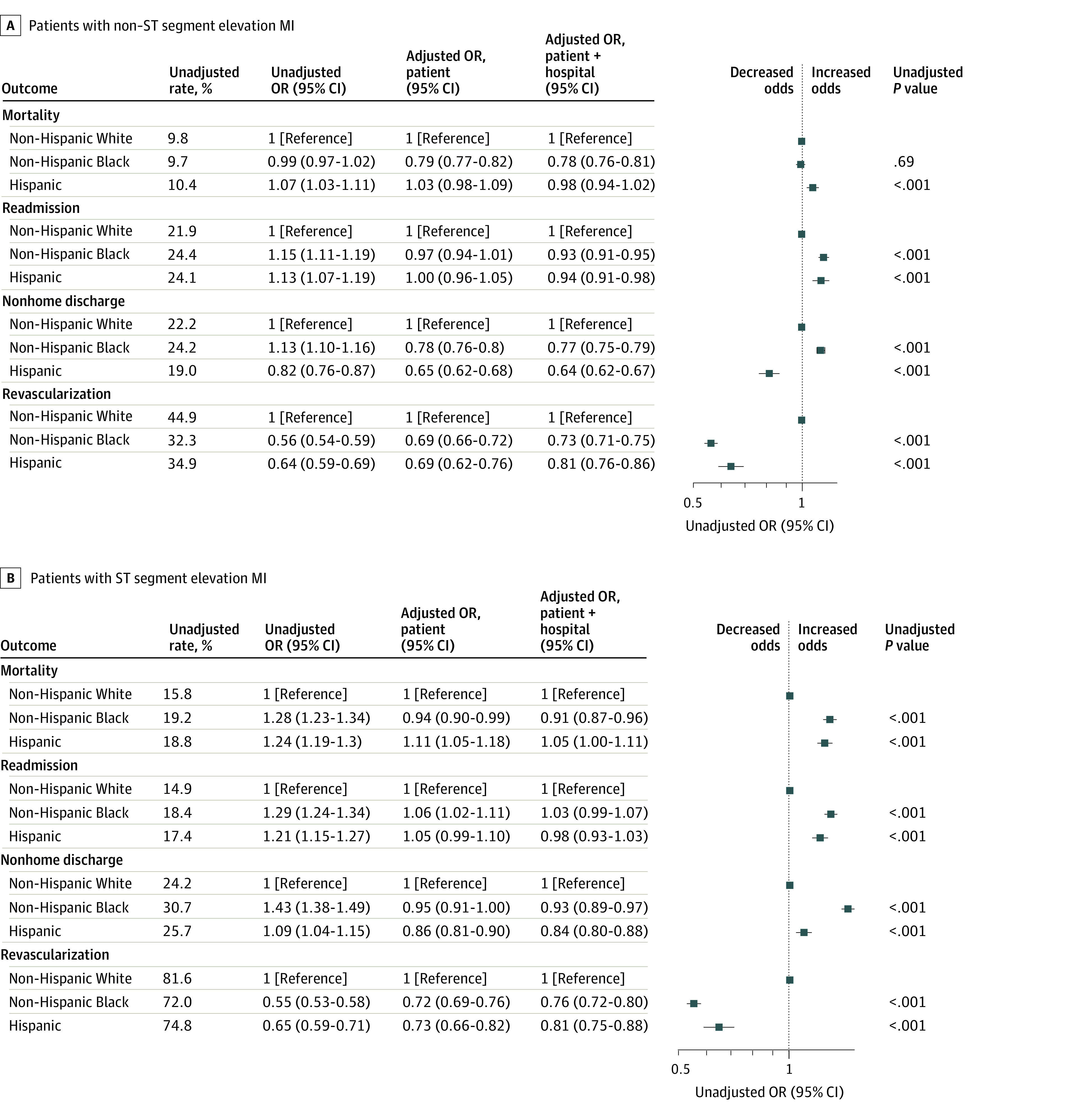
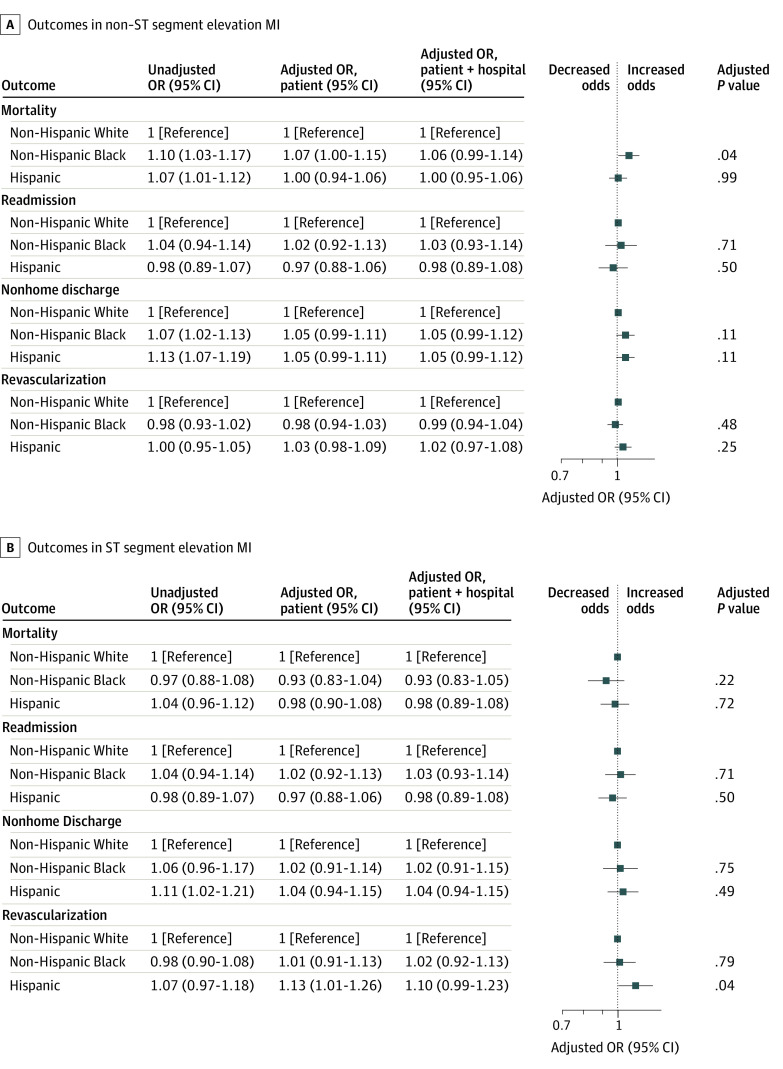
Results: A total of 1 319 273 admissions for AMI (579 817 females [44.0%]; 122 972 Black [9.3%], 117 668 Hispanic [8.9%], and 1 078 633 White [81.8%]; mean [SD] age, 77 [8.4] years) were included. For patients with non-ST segment elevation MI (NSTEMI) overall, the adjusted odds of mortality and nonhome discharges increased by 51% (adjusted odds ratio [aOR], 1.51; 95% CI, 1.29-1.76; P < .001) and 32% (aOR, 1.32; 95% CI, 1.15-1.52; P < .001), respectively, and the odds of revascularization decreased by 27% (aOR, 0.73; 95% CI, 0.64-0.83; P < .001) among patients hospitalized during weeks with a high hospital COVID-19 burden (>30%) vs patients hospitalized prior to the pandemic. Black individuals with NSTEMI experienced a clinically insignificant 7% greater increase in the odds of mortality (aOR, 1.07; 95% CI, 1.00-1.15; P = .04) for each 10% increase in the COVID-19 hospital burden but no increases in readmissions or nonhome discharges or reductions in revascularization rates compared with White individuals. There were no differential increases in adverse outcomes among Hispanic compared with White patients with NSTEMI based on hospital COVID-19 burden. Increases in hospital COVID-19 burden were not associated with changes in outcomes or the use of revascularization in STEMI overall or by racial or ethnic group.
Conclusions and relevance: This study found that while hospital COVID-19 burden was associated with worse treatment and outcomes for NSTEMI, race and ethnicity-associated inequities did not increase significantly during the pandemic. These findings suggest the need for additional efforts to mitigate outcomes associated with the COVID-19 pandemic for patients admitted with AMI when the hospital COVID-19 burden is substantially increased.
Conflict of interest statement
Figures
References
-
- Office of the Assistant Secretary for Planning and Evaluation . Impact of the COVID-19 pandemic on the hospital and outpatient clinician workforce. Department of Health and Human Services. Accessed December 12, 2022. https://aspe.hhs.gov/reports/covid-19-health-care-workforce
-
- Johns Hopkins University of Medicine . Coronavirus resource center. Accessed May 1, 2022. https://coronavirus.jhu.edu/map.html
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
