

Safety and efficacy of catheter ablation of atrial fibrillation in the very elderly (≥80 years old): Insights from the UC San Diego AF Ablation Registry
- PMID: 37626475
- PMCID: PMC10716336
- DOI: 10.1002/clc.24137
Safety and efficacy of catheter ablation of atrial fibrillation in the very elderly (≥80 years old): Insights from the UC San Diego AF Ablation Registry
Abstract
Background: Catheter ablation improves outcomes in symptomatic atrial fibrillation (AF) patients. However, its safety and efficacy in the very elderly (≥80 years old) is not well described.
Hypothesis: Ablation of AF in the very elderly is safe and effective.
Methods: We performed a retrospective study of all patients who underwent catheter ablation enrolled in the University of California, San Diego AF Ablation Registry. The primary outcome was freedom from atrial arrhythmias on or off antiarrhythmic drugs (AADs).
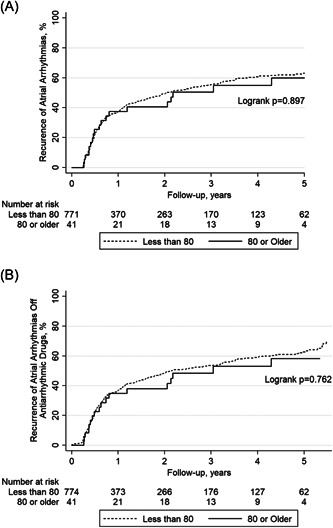
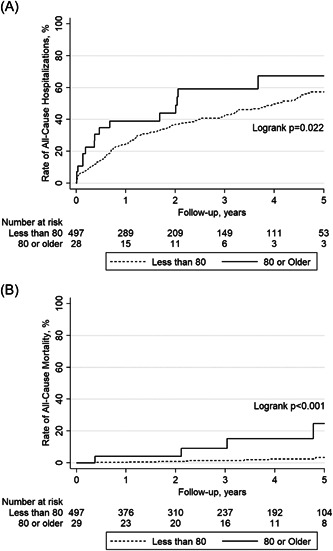
Results: Of 847 patients, 42 (5.0%) were 80 years of age or greater with a median age of 81.5 (80-82.3) and 805 (95.0%) were less than 80 years of age with a median age of 64.4 (57.6-70.2). Among those who were ≥80 years old, 29 were undergoing de novo ablation (69.0%), whereas in the younger cohort, 518 (64.5%) were undergoing de novo ablation (p = .548). There were no statistically significant differences in fluoroscopy (p = .406) or total procedure times (p = .076), AAD use (p = .611), or procedural complications (p = .500) between groups. After multivariable adjustment, there were no statistically significant differences in recurrence of any atrial arrhythmias on or off AAD (adjusted hazard ratio [AHR]: 0.75; 95% confidence interval [CI]: 0.45-1.23; p = .252), all-cause hospitalizations (AHR: 0.86; 95% CI: 0.46-1.60; p = .626), or all-cause mortality (AHR: 4.48; 95% CI: 0.59-34.07; p = .147) between the very elderly and the younger cohort.
Conclusion: In this registry analysis, catheter ablation of AF appears similarly effective and safe in patients 80 years or older when compared to a younger cohort.
Keywords: atrial fibrillation; catheter ablation; complications; hospitalizations; mortality; very elderly.
© 2023 The Authors. Clinical Cardiology published by Wiley Periodicals LLC.
Conflict of interest statement
Dr. Hsu reports receiving honoraria from Medtronic, Abbott, Boston Scientific, Biotronik, Janssen Pharmaceuticals, Bristol‐Myers Squibb, Pfizer, Sanofi, Zoll Medical, Hillrom, iRhythm, Acutus Medical, and Biosense‐Webster, equity interest in Vektor Medical, research grants from Biotronik and Biosense‐Webster, and research funding support from the Marouf Family and the Butler and Gratt family. Dr. Ho reports receiving a research grant from Abbott, equity in Vektor Medical, and fellowship support from Medtronic, Abbott, Boston Scientific, and Biotronik. Dr. Feld reports receiving fellowship training program stipends (as CCEP fellowship training program director) from Medtronic, Biotronik, Biosense Webster, and Abbott Medical, has equity interest in Vektor Medical, is co‐founder and co‐owner of Perminova, and is a consultant to Acutus Medical. Dr Han receives research support from Abbott and honoraria from Abbott. Dr. Aldaas, Dr. Darden, Dr. Mylavarapu, Amer Aldaas, Dr. Hoffmayer, Dr. Krummen, and Dr. Raissi have no conflicts of interest to disclose
Figures
Comment in
-
Efficacy and feasibility of catheter ablation in elderly patients with atrial fibrillation.Clin Cardiol. 2024 Feb;47(2):e24195. doi: 10.1002/clc.24195. Epub 2023 Nov 16. Clin Cardiol. 2024. PMID: 37970723 Free PMC article. No abstract available.
Similar articles
-
Association of isoproterenol infusion during catheter ablation of atrial fibrillation with outcomes: insights from the UC San Diego AF Ablation Registry.J Interv Card Electrophysiol. 2023 Aug;66(5):1243-1252. doi: 10.1007/s10840-022-01448-x. Epub 2022 Dec 12. J Interv Card Electrophysiol. 2023. PMID: 36508065 Free PMC article.
-
Comparison of Outcomes After Ablation of Atrial Fibrillation in Patients With Heart Failure With Preserved Versus Reduced Ejection Fraction.Am J Cardiol. 2020 Dec 1;136:62-70. doi: 10.1016/j.amjcard.2020.09.018. Epub 2020 Sep 15. Am J Cardiol. 2020. PMID: 32941815 Free PMC article.
-
Effect of Catheter Ablation Using Pulmonary Vein Isolation With vs Without Posterior Left Atrial Wall Isolation on Atrial Arrhythmia Recurrence in Patients With Persistent Atrial Fibrillation: The CAPLA Randomized Clinical Trial.JAMA. 2023 Jan 10;329(2):127-135. doi: 10.1001/jama.2022.23722. JAMA. 2023. PMID: 36625809 Free PMC article. Clinical Trial.
-
Catheter Ablation for Atrial Fibrillation in Elderly Patients: an Updated Meta-analysis of Comparative Studies.Can J Cardiol. 2024 Dec;40(12):2441-2451. doi: 10.1016/j.cjca.2024.08.263. Epub 2024 Aug 9. Can J Cardiol. 2024. PMID: 39127258
-
Catheter Ablation is Superior to Antiarrhythmic Drugs as First-Line Treatment for Atrial Fibrillation: a Systematic Review and Meta-Analysis.Arq Bras Cardiol. 2022 Jul;119(1):87-94. doi: 10.36660/abc.20210477. Arq Bras Cardiol. 2022. PMID: 35830118 Free PMC article. English, Portuguese.
Cited by
-
Disparities in the access to atrial fibrillation ablation in Denmark: who gets ablated, who neglected?Europace. 2024 Aug 30;26(9):euae231. doi: 10.1093/europace/euae231. Europace. 2024. PMID: 39230873 Free PMC article.
-
Efficacy and feasibility of catheter ablation in elderly patients with atrial fibrillation.Clin Cardiol. 2024 Feb;47(2):e24195. doi: 10.1002/clc.24195. Epub 2023 Nov 16. Clin Cardiol. 2024. PMID: 37970723 Free PMC article. No abstract available.
-
Temporal trends of catheter ablation procedures in patients with atrial fibrillation and atrial flutter: A nationwide cohort study.Int J Cardiol Heart Vasc. 2024 Oct 23;55:101541. doi: 10.1016/j.ijcha.2024.101541. eCollection 2024 Dec. Int J Cardiol Heart Vasc. 2024. PMID: 39507295 Free PMC article.
-
Safety and Outcomes of Catheter Ablation for Consecutive Atrial Tachycardia in Elderly Patients After Previous Cardiac Interventions.J Clin Med. 2025 Jan 21;14(3):675. doi: 10.3390/jcm14030675. J Clin Med. 2025. PMID: 39941346 Free PMC article.
-
Response to Letter to the Editor.Clin Cardiol. 2024 Feb;47(2):e24202. doi: 10.1002/clc.24202. Epub 2023 Dec 19. Clin Cardiol. 2024. PMID: 38112162 Free PMC article. No abstract available.
References
-
- Colilla S, Crow A, Petkun W, Singer DE, Simon T, Liu X. Estimates of current and future incidence and prevalence of atrial fibrillation in the U.S. adult population. Am J Cardiol. 2013;112:1142‐1147. - PubMed
-
- Go AS, Hylek EM, Phillips KA, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) study. JAMA. 2001;285:2370‐2375. - PubMed
-
- January CT, Wann LS, Calkins H, et al. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation. Circulation. 2019;140:e125‐e151. - PubMed
-
- Kirchhof P, Camm AJ, Goette A, et al. Early rhythm‐control therapy in patients with atrial fibrillation. N Engl J Med. 2020;383:1305‐1316. - PubMed
-
- Chatap G, Giraud K, Vincent JP. Atrial fibrillation in the elderly: facts and management. Drugs Aging. 2002;19:819‐846. - PubMed
