

Neurological Insights into Sleep Disorders in Parkinson's Disease
- PMID: 37626558
- PMCID: PMC10452387
- DOI: 10.3390/brainsci13081202
Neurological Insights into Sleep Disorders in Parkinson's Disease
Abstract
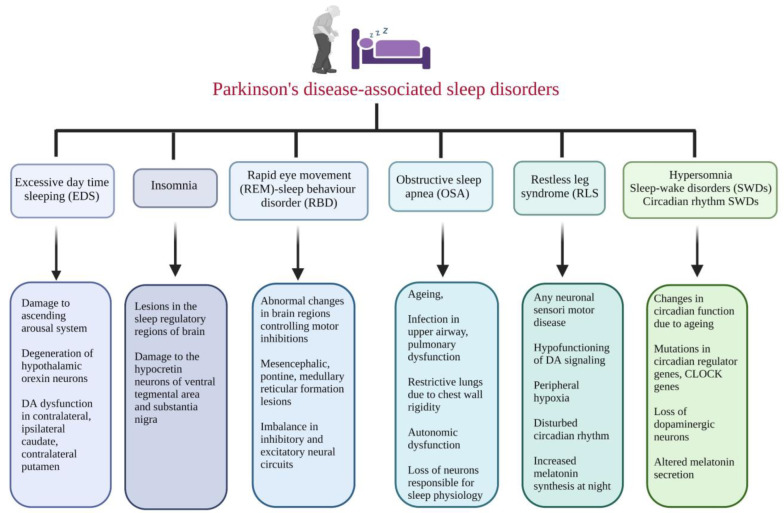
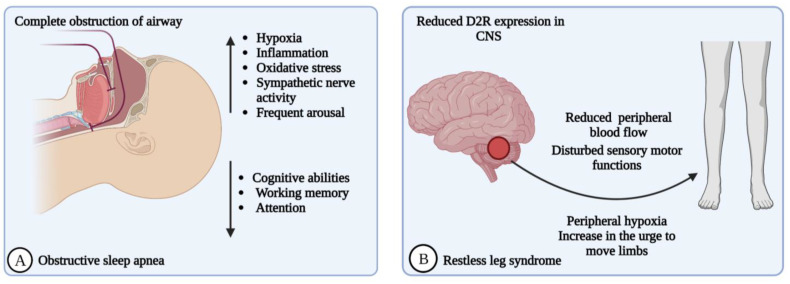
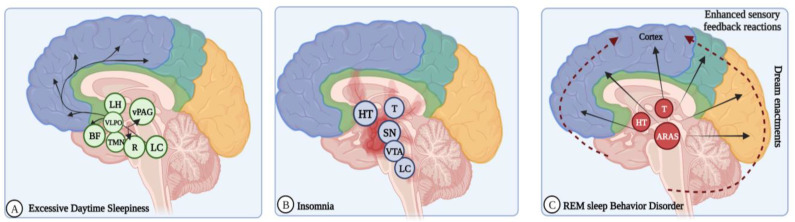
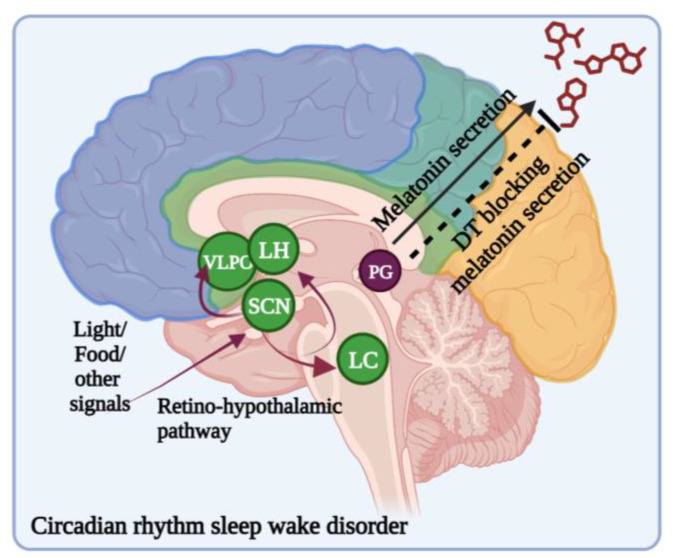
Parkinson's disease (PD) is a common multidimensional neurological disorder characterized by motor and non-motor features and is more prevalent in the elderly. Sleep disorders and cognitive disturbances are also significant characteristics of PD. Sleep is an important physiological process for normal human cognition and physical functioning. Sleep deprivation negatively impacts human physical, mental, and behavioral functions. Sleep disturbances include problems falling asleep, disturbances occurring during sleep, abnormal movements during sleep, insufficient sleep, and excessive sleep. The most recognizable and known sleep disorders, such as rapid-eye-movement behavior disorder (RBD), insomnia, excessive daytime sleepiness (EDS), restless legs syndrome (RLS), sleep-related breathing disorders (SRBDs), and circadian-rhythm-related sleep-wake disorders (CRSWDs), have been associated with PD. RBD and associated emotional disorders are common non-motor symptoms of PD. In individuals, sleep disorders and cognitive impairment are important prognostic factors for predicting progressing neurodegeneration and developing dementia conditions in PD. Studies have focused on RBD and its associated neurological changes and functional deficits in PD patients. Other risks, such as cognitive decline, anxiety, and depression, are related to RBD. Sleep-disorder diagnosis is challenging, especially in identifying the essential factors that disturb the sleep-wake cycle and the co-existence of other concomitant sleep issues, motor symptoms, and breathing disorders. Focusing on sleep patterns and their disturbances, including genetic and other neurochemical changes, helps us to better understand the central causes of sleep alterations and cognitive functions in PD patients. Relations between α-synuclein aggregation in the brain and gender differences in sleep disorders have been reported. The existing correlation between sleep disorders and levels of α-synuclein in the cerebrospinal fluid indicates the risk of progression of synucleinopathies. Multidirectional approaches are required to correlate sleep disorders and neuropsychiatric symptoms and diagnose sensitive biomarkers for neurodegeneration. The evaluation of sleep pattern disturbances and cognitive impairment may aid in the development of novel and effective treatments for PD.
Keywords: Parkinson’s disease; circadian rhythm; excessive daytime sleepiness; insomnia; rapid eye movement; sleep disorders; sleep-related breathing disorders.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
[Selective stimulations and lesions of the rat brain nuclei as the models for research of the human sleep pathology mechanisms].Glas Srp Akad Nauka Med. 2011;(51):85-97. Glas Srp Akad Nauka Med. 2011. PMID: 22165729 Review. Serbian.
-
Sleep Issues in Parkinson's Disease and Their Management.Neurotherapeutics. 2020 Oct;17(4):1480-1494. doi: 10.1007/s13311-020-00938-y. Epub 2020 Oct 7. Neurotherapeutics. 2020. PMID: 33029723 Free PMC article. Review.
-
The Genetic Landscape of Sleep Disorders in Parkinson's Disease.Diagnostics (Basel). 2024 Jan 3;14(1):106. doi: 10.3390/diagnostics14010106. Diagnostics (Basel). 2024. PMID: 38201415 Free PMC article. Review.
-
Sleep disturbances in Parkinson's disease with emphasis on rapid eye movement sleep behavior disorder.Int J Neurosci. 2012 Aug;122(8):407-12. doi: 10.3109/00207454.2012.677882. Epub 2012 May 11. Int J Neurosci. 2012. PMID: 22463496
-
Factors contributing to sleep disturbances and excessive daytime sleepiness in patients with Parkinson's disease.Front Neurol. 2023 Mar 9;14:1097251. doi: 10.3389/fneur.2023.1097251. eCollection 2023. Front Neurol. 2023. PMID: 36970510 Free PMC article.
Cited by
-
Short-Term Therapeutic Effect of Repetitive Transcranial Magnetic Stimulations of Sleep Disorders in Parkinson's Disease: A Randomized Clinical Trial (Pilot Study).Brain Sci. 2024 May 30;14(6):556. doi: 10.3390/brainsci14060556. Brain Sci. 2024. PMID: 38928556 Free PMC article.
-
Prevalence and associations of self-reported sleep problems in a large sample of patients with Parkinson's disease.J Sleep Res. 2025 Aug;34(4):e14453. doi: 10.1111/jsr.14453. Epub 2025 Jan 19. J Sleep Res. 2025. PMID: 39828248 Free PMC article.
-
Sleep Disturbances and Pain Subtypes in Parkinson's Disease.Medicina (Kaunas). 2025 Mar 26;61(4):591. doi: 10.3390/medicina61040591. Medicina (Kaunas). 2025. PMID: 40282882 Free PMC article.
-
Sleep duration in middle-aged years of life predicts the age of diagnosis of Parkinson's disease.Sleep Med X. 2024 Aug 16;8:100123. doi: 10.1016/j.sleepx.2024.100123. eCollection 2024 Dec 15. Sleep Med X. 2024. PMID: 39263596 Free PMC article.
-
Non-motor symptoms of Parkinson`s disease-insights from genetics.J Neural Transm (Vienna). 2024 Nov;131(11):1277-1284. doi: 10.1007/s00702-024-02833-8. Epub 2024 Sep 19. J Neural Transm (Vienna). 2024. PMID: 39294309 Review.
References
-
- Radhakrishnan D.M., Goyal V. Parkinson’s disease. A review. Neurol. India. 2018;66:26–35. - PubMed
-
- Baldereschi M., Di Carlo A., Rocca W.A., Vanni P., Maggi S., Perissinotto E. Parkinson’s disease and Parkinsonism in a longitudinal study: Two-fold higher incidence in men. ILSA Working Group. Italian Longitudinal Study on Aging. Neurology. 2000;55:1358–1363. doi: 10.1212/WNL.55.9.1358. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
