

Trends in Dual Antiplatelet Therapy Use for Neurointerventional Procedures for the Management of Intracranial Aneurysms
- PMID: 37626730
- PMCID: PMC10452183
- DOI: 10.3390/biomedicines11082234
Trends in Dual Antiplatelet Therapy Use for Neurointerventional Procedures for the Management of Intracranial Aneurysms
Abstract
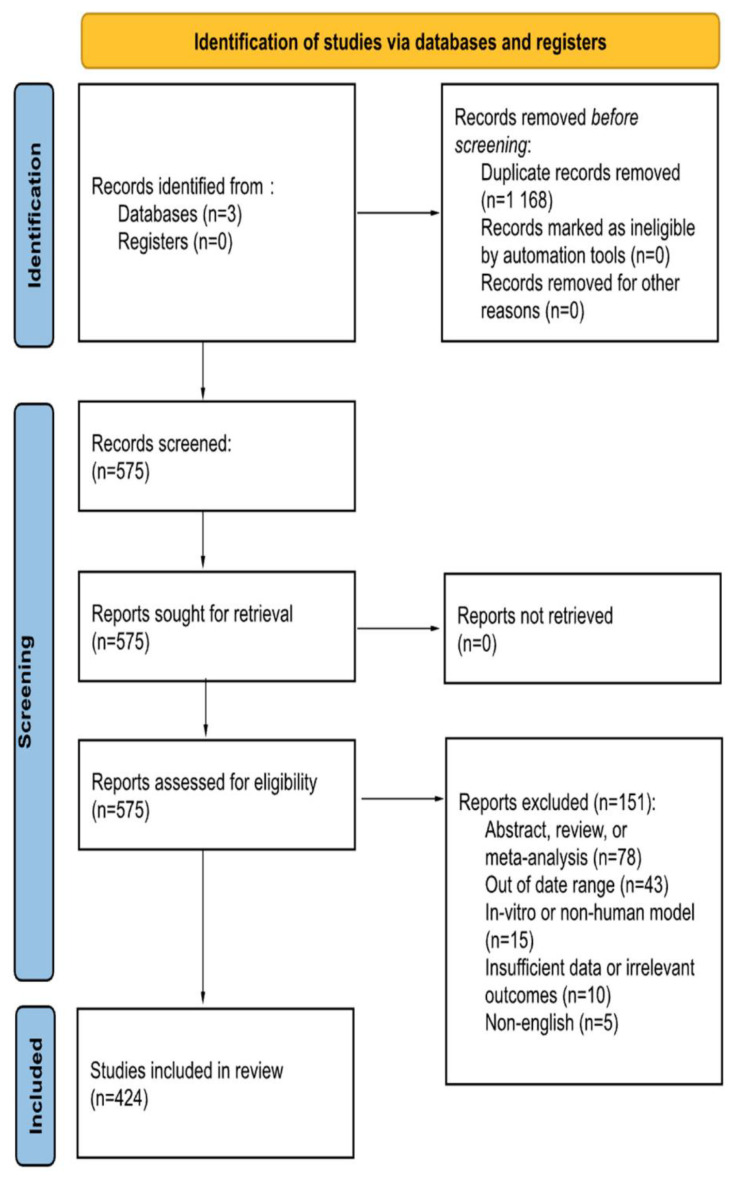
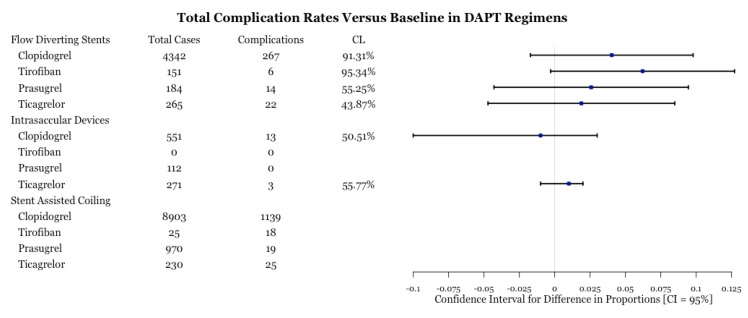
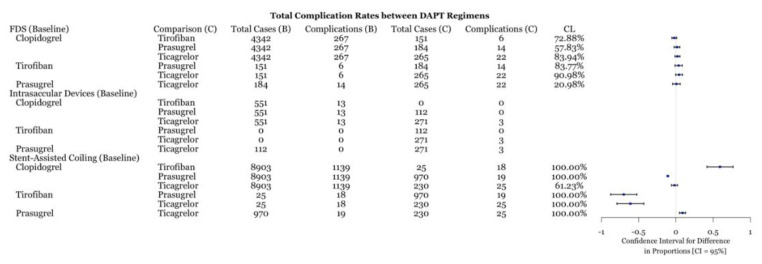
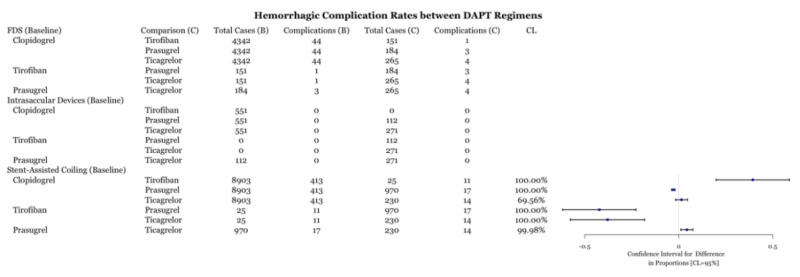
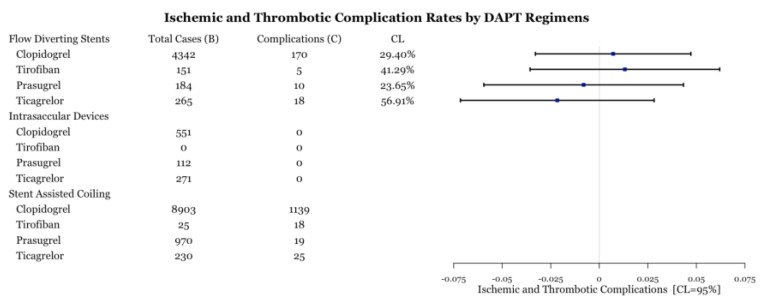
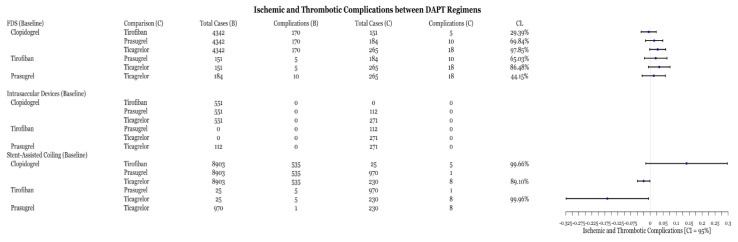
The use of periprocedural dual antiplatelet therapy (DAPT) has significantly evolved along with innovations in the endovascular management of intracranial aneurysms. Historically, aspirin and clopidogrel have been the most commonly employed regimen due to its safety and efficacy. However, recent studies highlight the importance of tailoring DAPT regimens to individual patient characteristics which may affect clopidogrel metabolism, such as genetic polymorphisms. In the present report, a systematic review of the literature was performed to determine optimal antiplatelet use with flow diverting stents, intracranial stents, intrasaccular devices, and stent-assisted coiling. Studies were analyzed for the number of aneurysms treated, DAPT regimen, and any thromboembolic complications. Based on inclusion criteria, 368 studies were selected, which revealed the increasing popularity of alternative DAPT regimens with the aforementioned devices. Thromboembolic or hemorrhagic complications associated with antiplatelet medications were similar across all medications. DAPT with ticagrelor, tirofiban, or prasugrel are effective and safe alternatives to clopidogrel and do not require enzymatic activation. Further clinical trials are needed to evaluate different antiplatelet regimens with various devices to establish highest-level evidence-based guidelines and recommendations.
Keywords: dual antiplatelet therapy; flow diverting stents; intracranial aneurysm; intracranial stenting; monotherapy; stent-assisted coiling.
Conflict of interest statement
Alexander L. Coon is a consultant for Medtronic Neurovascular, MicroVention-Terumo, Stryker Neurovascular, Rapid Medical; and a consultant for Avail MedSystems, Imperative Care, InNeuroCo, Medtronic Neurovascular, MicroVention-Terumo, Q’apel, Rapid Medical, Stryker Neurovascular, and Sequent Medical; a proctor for MicroVention-Termo, Stryker Neurovascular, and Medtronic Neurovascular. All other authors have no conflict of interest. No author received financial support in conjunction with the generation of this submission.
Figures
References
-
- Steinhubl S.R., Berger P.B., Iii J.T.M., Fry E.T.A., Delago A., Wilmer C., Topol E., CREDO Investigators Early and Sustained Dual Oral Antiplatelet Therapy Following Percutaneous Coronary Intervention: A Randomized Controlled Trial. JAMA. 2002;288:2411–2420. doi: 10.1001/jama.288.19.2411. Erratum in JAMA 2003, 289, 987. - DOI - PubMed
