

Surgical Anatomy of the Gastrointestinal Tract in Cats
- PMID: 37627461
- PMCID: PMC10451872
- DOI: 10.3390/ani13162670
Surgical Anatomy of the Gastrointestinal Tract in Cats
Abstract
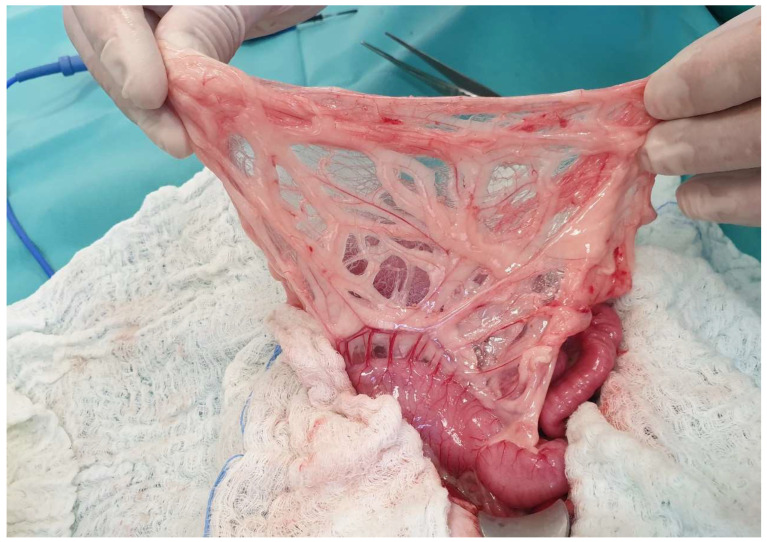
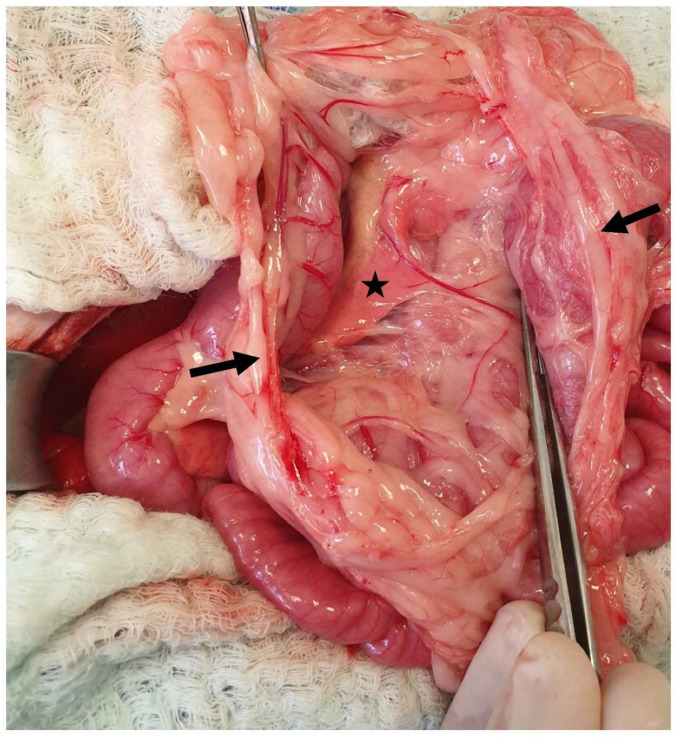
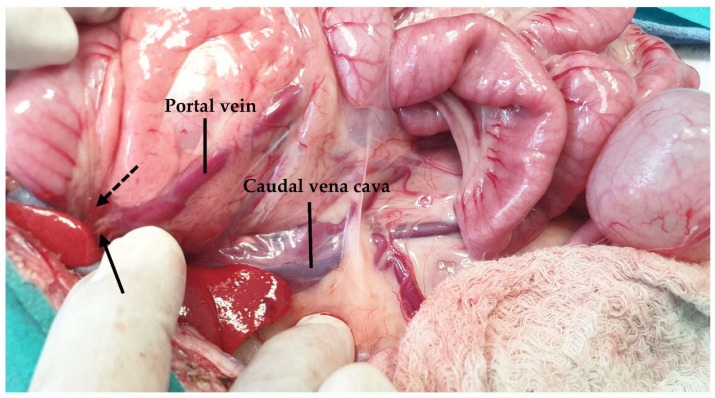
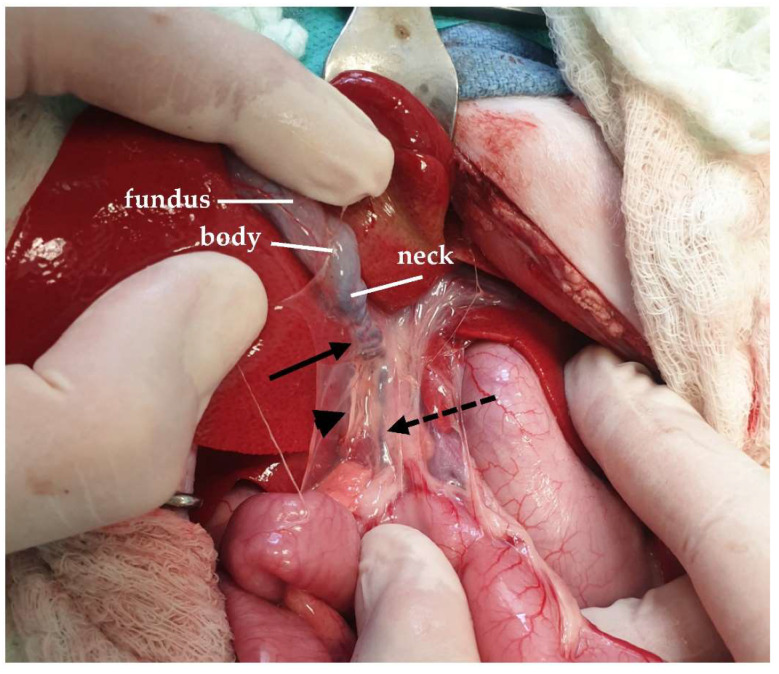
In cats, the gastrointestinal tract is one of the regions in which surgical procedures are most frequently performed by veterinary surgeons; therefore, knowledge of the surgical anatomy of the feline gastrointestinal tract is of high importance. The main surgical procedures performed include gastrotomy, gastrectomy, enterotomy, and enterectomy, as well as procedures in the liver and pancreas. There are also anatomical differences between dogs and cats, increasing the need for deep knowledge of the anatomy treated in the different surgical approaches. The aim of the present review is to describe in detail the anatomy of the gastrointestinal tract in cats highlighting the anatomical regions of significant importance in different surgical procedures.
Keywords: abdomen; anatomy; feline; gastrointestinal surgery.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



Similar articles
-
Rabbit Soft Tissue Surgery.Vet Clin North Am Exot Anim Pract. 2016 Jan;19(1):159-88. doi: 10.1016/j.cvex.2015.08.007. Vet Clin North Am Exot Anim Pract. 2016. PMID: 26611928 Review.
-
Preliminary Studies on the Intrahepatic Anatomy of the Venous Vasculature in Cats.Vet Sci. 2022 Nov 2;9(11):607. doi: 10.3390/vetsci9110607. Vet Sci. 2022. PMID: 36356084 Free PMC article.
-
Surgical stapling of the spleen, pancreas, liver, and urogenital tract.Vet Clin North Am Small Anim Pract. 1994 Mar;24(2):375-94. doi: 10.1016/s0195-5616(94)50158-x. Vet Clin North Am Small Anim Pract. 1994. PMID: 8197676 Review.
-
Effects of a surgical checklist on decreasing incisional infections following foreign body removal from the gastrointestinal tract in dogs.Can Vet J. 2019 Jan;60(1):67-72. Can Vet J. 2019. PMID: 30651653 Free PMC article.
-
Clinical outcomes of the use of unidirectional barbed sutures in gastrointestinal surgery for dogs and cats: A retrospective study.Vet Surg. 2023 Oct;52(7):1009-1014. doi: 10.1111/vsu.13978. Epub 2023 Jun 18. Vet Surg. 2023. PMID: 37332126
Cited by
-
Lesions Distribution, Nature and Severity Along the Gastrointestinal Tract in Cats With Low-Grade Intestinal T-Cell Lymphoma or Lymphoplasmacytic Enteritis.J Vet Intern Med. 2025 Sep-Oct;39(5):e70148. doi: 10.1111/jvim.70148. J Vet Intern Med. 2025. PMID: 40767104 Free PMC article.
References
-
- Langley-Hobbs S.J., Demetriou J.L., Ladlow J.F. Preface. In: Langley-Hobbs S.J., Demetriou J., Ladlow J.F., editors. Feline Soft Tissue and General Surgery. Elsevier; London, UK: 2014. p. ix.
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
