Locoregional Therapies and Remodeling of Tumor Microenvironment in Pancreatic Cancer
- PMID: 37628865
- PMCID: PMC10454061
- DOI: 10.3390/ijms241612681
Locoregional Therapies and Remodeling of Tumor Microenvironment in Pancreatic Cancer
Abstract
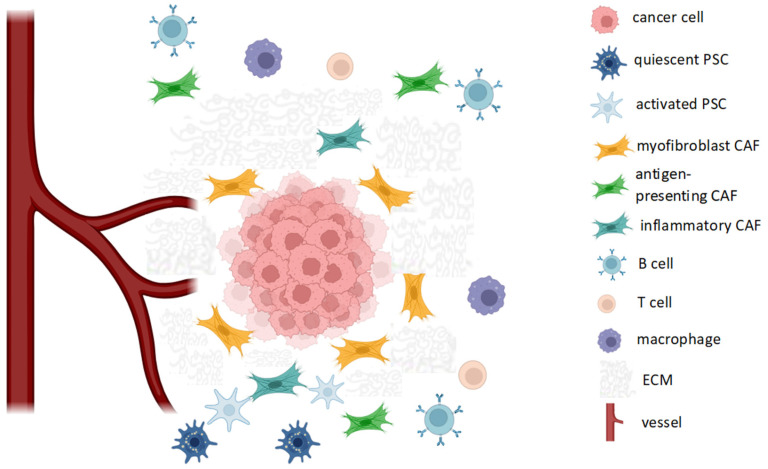
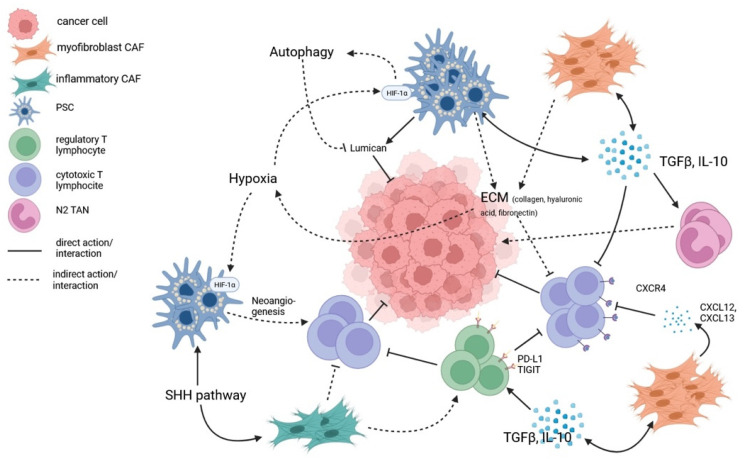
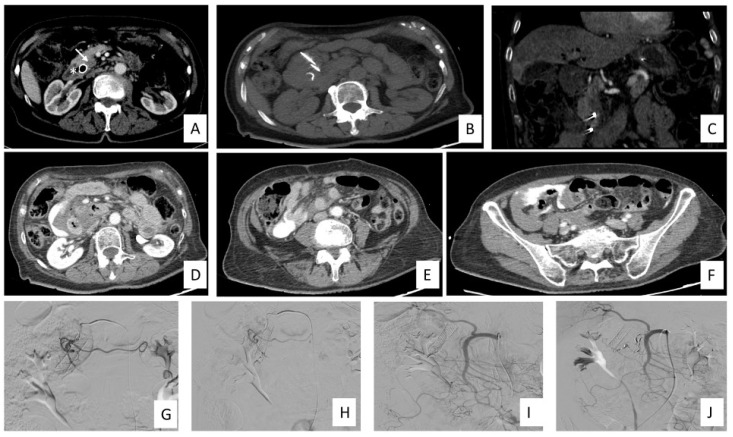
Despite the advances made in treatment, the prognosis of pancreatic ductal adenocarcinoma (PDAC) remains dismal, even in the locoregional and locally advanced stages, with high relapse rates after surgery. PDAC exhibits a chemoresistant and immunosuppressive phenotype, and the tumor microenvironment (TME) surrounding cancer cells actively participates in creating a stromal barrier to chemotherapy and an immunosuppressive environment. Recently, there has been an increasing use of interventional radiology techniques for the treatment of PDAC, although they do not represent a standard of care and are not included in clinical guidelines. Local approaches such as radiation therapy, hyperthermia, microwave or radiofrequency ablation, irreversible electroporation and high-intensity focused ultrasound exert their action on the tumor tissue, altering the composition and structure of TME and potentially enhancing the action of chemotherapy. Moreover, their action can increase antigen release and presentation with T-cell activation and reduction tumor-induced immune suppression. This review summarizes the current evidence on locoregional therapies in PDAC and their effect on remodeling TME to make it more susceptible to the action of antitumor agents.
Keywords: ablation therapies; locoregional treatments; pancreatic cancer; radiotherapy; tumor microenvironment.
Conflict of interest statement
The authors declare no conflict of interest.
Figures