

Unveiling the Challenges in Tandem Ureteral Stent Management for Malignant Ureteral Obstruction: Failure Rate, Risk Factors, and Durability of Their Replacement
- PMID: 37629293
- PMCID: PMC10455996
- DOI: 10.3390/jcm12165251
Unveiling the Challenges in Tandem Ureteral Stent Management for Malignant Ureteral Obstruction: Failure Rate, Risk Factors, and Durability of Their Replacement
Abstract
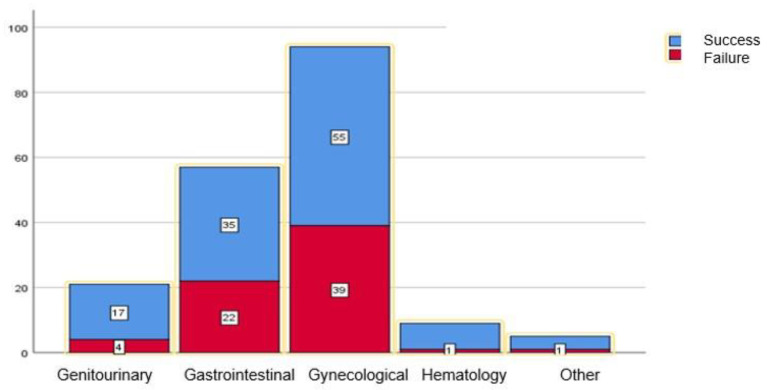
Background: Malignant ureteral obstruction (MUO) is a sequela of advanced malignant disease that requires renal drainage, with tandem ureteral stents (TUSs) being a viable option. This study aimed to evaluate the TUS failure rate, associated risk factors, and the feasibility of replacing failed TUSs with a new pair of stents.
Methods: A retrospective analysis of MUO patients treated with TUS insertion from 2014 to 2022 was conducted. TUS failure was defined as urosepsis, recurrent urinary tract infections, acute kidney failure, or new hydronephrosis on imaging. Cox proportional hazard regression analysis identified the independent predictors of TUS failure.
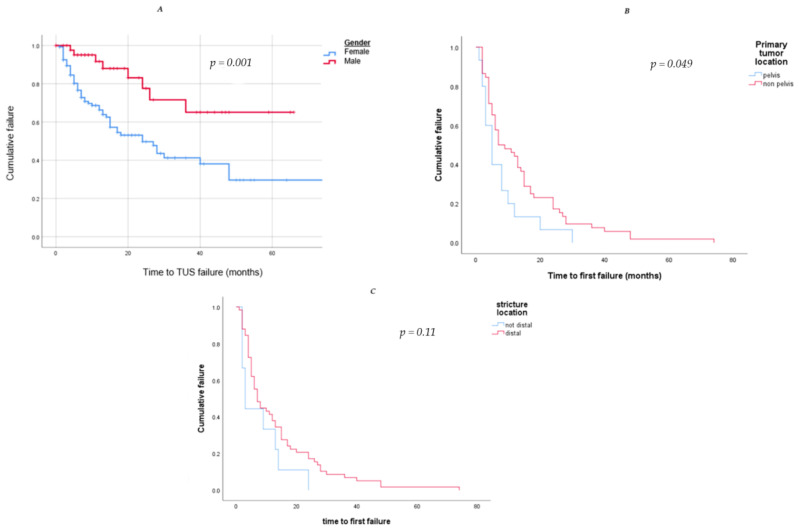
Results: A total of 240 procedures were performed on 186 patients, with TUS drainage failing in 67 patients (36%). The median time to failure was 7 months. Multivariate analysis revealed female gender (OR = 3.46, p = 0.002), pelvic mass (OR = 1.75, p = 0.001), and distal ureteral obstruction (OR = 2.27, p = 0.04) as significant risk factors for TUS failure. Of the failure group, 42 patients (22.6%) underwent TUS replacement for a new pair. Yet, 24 (57.2%) experienced a second failure, with a median time of 4.5 months. The risk factors for TUS second failure included a stricture longer than 30 mm (OR = 11.8, p = 0.04), replacement with TUSs of the same diameter (OR = 43, p = 0.003), and initial TUS failure within 6 months (OR = 19.2, p = 0.006).
Conclusions: TUS insertion for the treatment of MUO is feasible and has good outcomes with a relatively low failure rate. Primary pelvic mass and distal ureteral obstruction pose higher risks for TUS failure. Replacing failed TUSs with a new pair has a success rate of 42.8%. Consideration should be given to placing larger diameter stents when replacing failed TUS.
Keywords: malignant ureteral obstruction; polymeric stents; renal drainage; tandem ureteral stents; ureteral stricture.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



References
-
- Plesinac-Karapandzic V., Masulovic D., Markovic B., Djuric-Stefanovic A., Plesinac S., Vucicevic D., Milovanovic Z., Milosevic Z. Percutaneous nephrostomy in the management of advanced and terminal-stage gynecologic malignancies: Outcome and complications. Eur. J. Gynaecol. Oncol. 2010;31:645–650. - PubMed
LinkOut - more resources
Full Text Sources
