

Long-Term Outcomes of Birdshot Chorioretinopathy Treated with Corticosteroids: A Case Reports
- PMID: 37629330
- PMCID: PMC10455668
- DOI: 10.3390/jcm12165288
Long-Term Outcomes of Birdshot Chorioretinopathy Treated with Corticosteroids: A Case Reports
Abstract
Purpose: To report the progression of patients diagnosed with birdshot chorioretinopathy (BSCR) initially treated with corticosteroids.
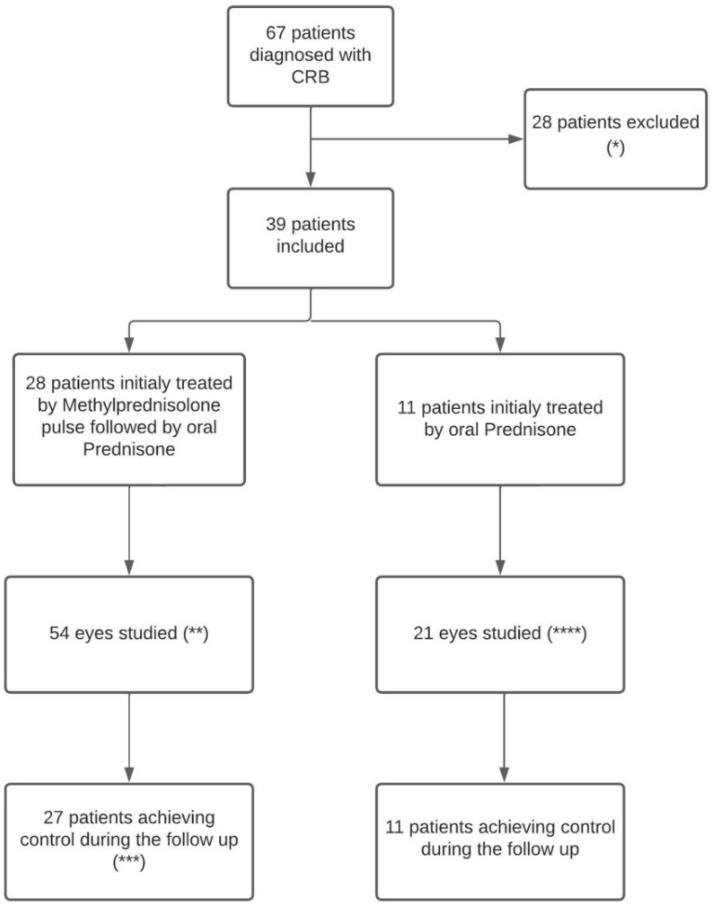
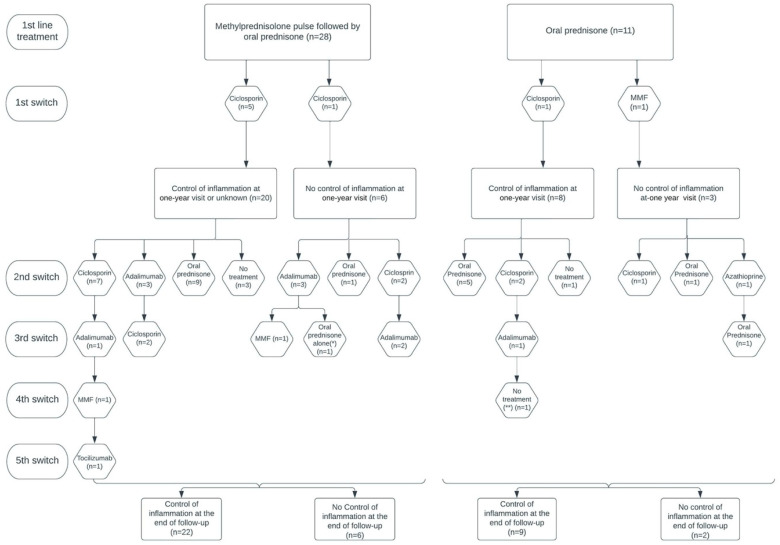
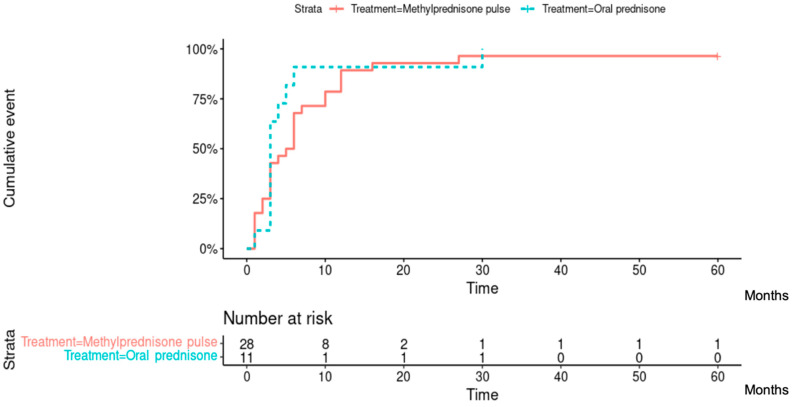
Methods: We included 39 BSCR patients that were followed for ≥1 year. We analyzed their progression under treatment after 1, 3, 6 months, 1 year, and at the end of follow-up. In order to determine the efficiency of initial loading doses, patients were classified into two groups according to their initial treatment: methylprednisolone followed by prednisone (n = 28) and prednisone alone (n = 11).
Results: At the end of follow-up, 31/39 (79.5%) patients had reached inflammation control. Thirteen out of 28 (46.4%) and 6/11 (54.5%) patients were treated exclusively with corticosteroids, and 18/19 (94.7%) of them had reached inflammation control at the end of follow-up; their mean (range) corticosteroid dose was 3.5 (0-10) mg/day.
Conclusions: We found that the prolonged corticosteroid therapy treatment strategy resulted in inflammation control in half of BSCR patients. This control was maintained with low doses of cortisone, usually <5 mg/day.
Keywords: birdshot chorioretinopathy (BSCR); corticosteroids; inflammatory macular edema; prognosis; relapse; uveitis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Gelfman S., Monnet D., Ligocki A.J., Tabary T., Moscati A., Bai X., Freudenberg J., Cooper B., Kosmicki J.A., Wolf S., et al. ERAP1, ERAP2, and Two Copies of HLA-Aw19 Alleles Increase the Risk for Birdshot Chorioretinopathy in HLA-A29 Carriers. Investig. Ophthalmol. Vis. Sci. 2021;62:3. doi: 10.1167/iovs.62.14.3. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
