

Is the Combination of Plain X-ray and Probe-to-Bone Test Useful for Diagnosing Diabetic Foot Osteomyelitis? A Systematic Review and Meta-Analysis
- PMID: 37629412
- PMCID: PMC10455253
- DOI: 10.3390/jcm12165369
Is the Combination of Plain X-ray and Probe-to-Bone Test Useful for Diagnosing Diabetic Foot Osteomyelitis? A Systematic Review and Meta-Analysis
Abstract
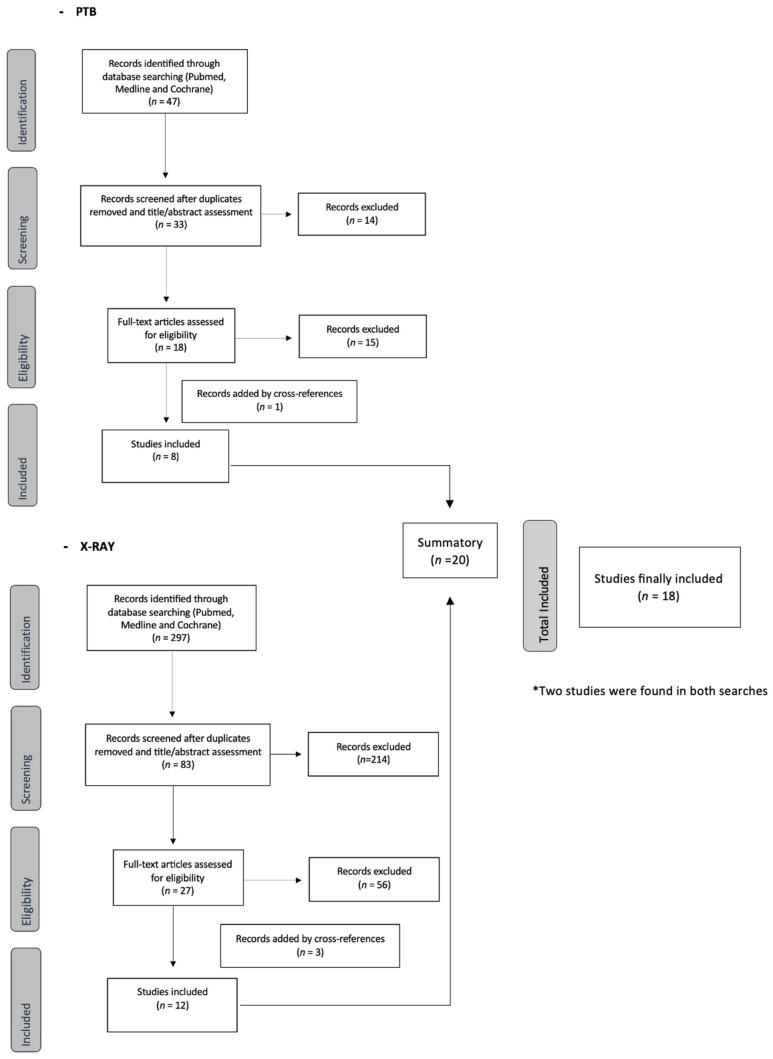
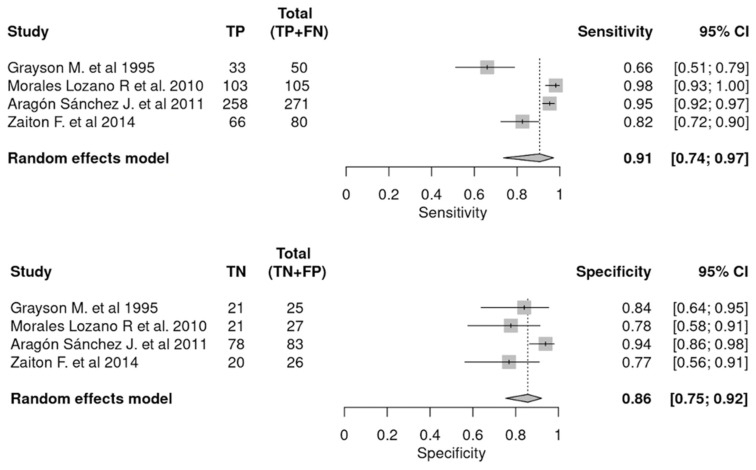
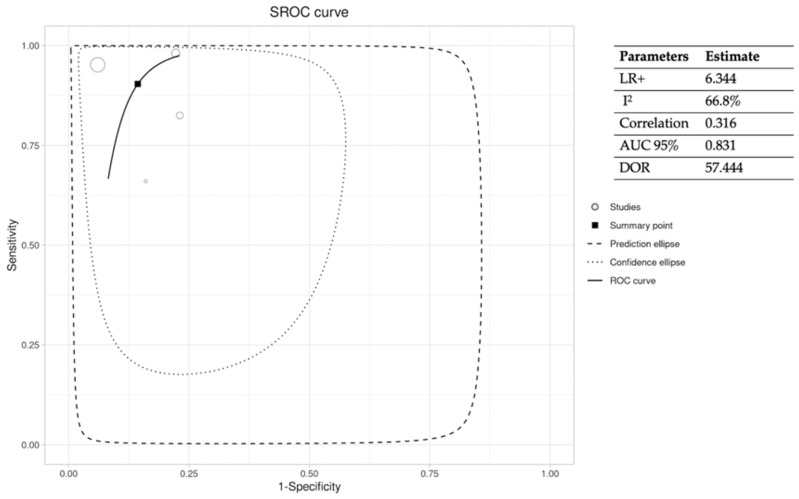
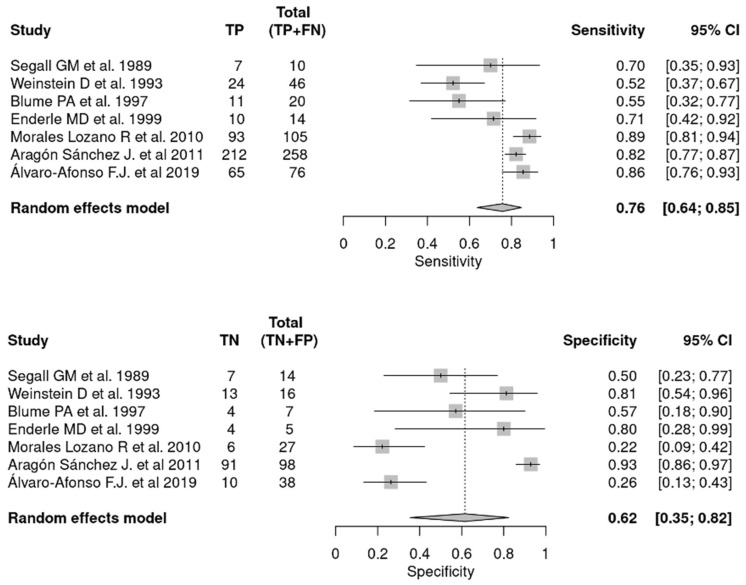
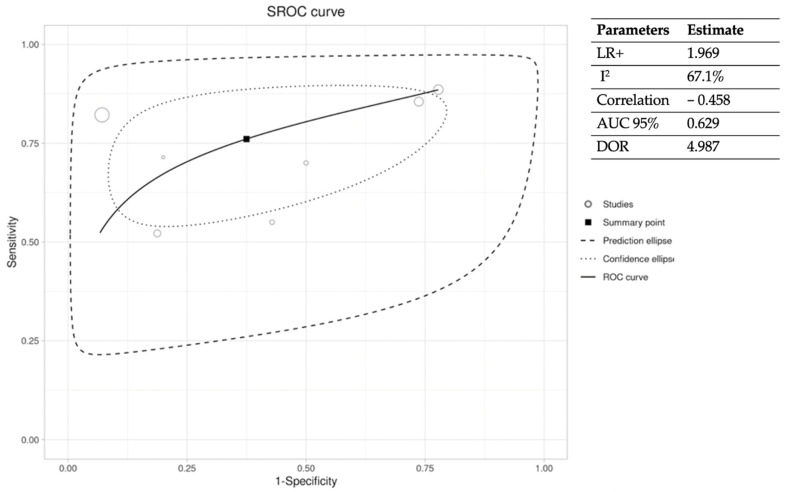
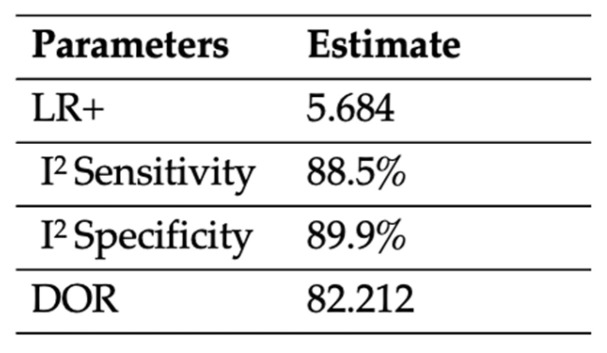
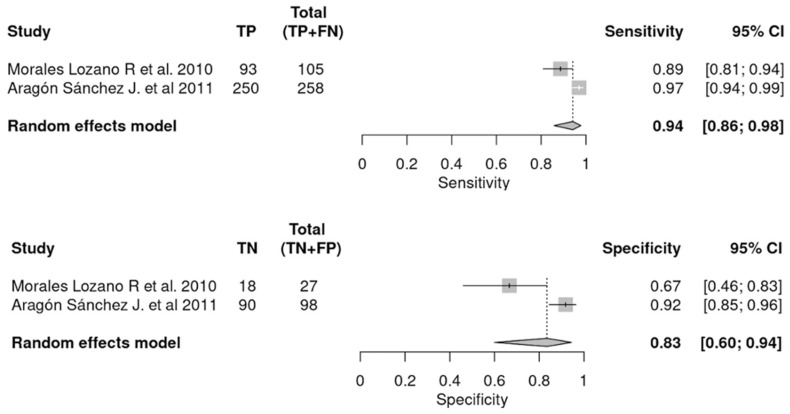
A systematic review and meta-analysis was conducted to assess the diagnostic accuracy of the combination of plain X-ray and probe-to-bone (PTB) test for diagnosing diabetic foot osteomyelitis (DFO). This systematic review has been registered in PROSPERO (a prospective international register of systematic reviews; identification code CRD42023436757). A literature search was conducted for each test separately along with a third search for their combination. A total of 18 articles were found and divided into three groups for separate analysis and comparison. All selected studies were evaluated using STROBE guidelines to assess the quality of reporting for observational studies. Meta-DiSc software was used to analyze the collected data. Concerning the diagnostic accuracy variables for each case, the pooled sensitivity (SEN) was higher for the combination of PTB and plain X-ray [0.94 (PTB + X-ray) vs. 0.91 (PTB) vs. 0.76 (X-ray)], as was the diagnostic odds ratio (DOR) (82.212 (PTB + X-ray) vs. 57.444 (PTB) vs. 4.897 (X-ray)). The specificity (SPE) and positive likelihood ratio (LR+) were equally satisfactory for the diagnostic combination but somewhat lower than for PTB alone (SPE: 0.83 (PTB + X-ray) vs. 0.86 (PTB) vs. 0.76 (X-ray); LR+: 5.684 (PTB + X-ray) vs. 6.344 (PTB) vs. 1.969 (X-ray)). The combination of PTB and plain X-ray showed high diagnostic accuracy comparable to that of MRI and histopathology diagnosis (the gold standard), so it could be considered useful for the diagnosis of DFO. In addition, this diagnostic combination is accessible and inexpensive but requires training and experience to correctly interpret the results. Therefore, recommendations for this technique should be included in the context of specialized units with a high prevalence of DFO.
Keywords: diabetic foot; diabetic foot osteomyelitis; diabetic foot ulcer; plain X-ray; probe-to-bone test.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Diagnosing diabetic foot osteomyelitis: is the combination of probe-to-bone test and plain radiography sufficient for high-risk inpatients?Diabet Med. 2011 Feb;28(2):191-4. doi: 10.1111/j.1464-5491.2010.03150.x. Diabet Med. 2011. PMID: 21219428
-
Validating the probe-to-bone test and other tests for diagnosing chronic osteomyelitis in the diabetic foot.Diabetes Care. 2010 Oct;33(10):2140-5. doi: 10.2337/dc09-2309. Epub 2010 Jul 9. Diabetes Care. 2010. PMID: 20622159 Free PMC article.
-
Does this patient with diabetes have osteomyelitis of the lower extremity?JAMA. 2008 Feb 20;299(7):806-13. doi: 10.1001/jama.299.7.806. JAMA. 2008. PMID: 18285592 Review.
-
Diagnosing diabetic foot osteomyelitis.Diabetes Metab Res Rev. 2020 Mar;36 Suppl 1:e3250. doi: 10.1002/dmrr.3250. Epub 2020 Jan 17. Diabetes Metab Res Rev. 2020. PMID: 31950555
-
Clinical Inquiry: What's the best test for underlying osteomyelitis in patients with diabetic foot ulcers?J Fam Pract. 2015 May;64(5):309-10, 321. J Fam Pract. 2015. PMID: 26009740 Review.
Cited by
-
Diagnostic Performance of Atherogenic Index of Plasma for Predicting Diabetic Foot Osteomyelitis with Peripheral Artery Disease.J Clin Med. 2024 Mar 27;13(7):1934. doi: 10.3390/jcm13071934. J Clin Med. 2024. PMID: 38610699 Free PMC article.
References
-
- Prompers L., Huijberts M., Apelqvist J., Jude E., Piaggesi A., Bakker K., Edmonds M., Holstein P., Jirkovska A., Mauricio D., et al. High prevalence of ischaemia, infection and serious comorbidity in patients with diabetic foot disease in Europe. Baseline results from the Eurodiale study. Diabetologia. 2007;50:18–25. doi: 10.1007/s00125-006-0491-1. - DOI - PubMed
-
- Lipsky B.A., Berendt A.R., Cornia P.B., Pile J.C., Peters E.J., Armstrong D.G., Deery H.G., Embil J.M., Joseph W., Karchmer A., et al. 2012 infectious diseases society of America clinical practice guideline for the diagnosis and treatment of diabetic foot infections. Clin. Infect. Dis. 2012;54:132–173. doi: 10.1093/cid/cis346. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
