

Impact of Persistent Inflammation, Immunosuppression, and Catabolism Syndrome during Intensive Care Admission on Each Post-Intensive Care Syndrome Component in a PICS Clinic
- PMID: 37629468
- PMCID: PMC10455637
- DOI: 10.3390/jcm12165427
Impact of Persistent Inflammation, Immunosuppression, and Catabolism Syndrome during Intensive Care Admission on Each Post-Intensive Care Syndrome Component in a PICS Clinic
Abstract
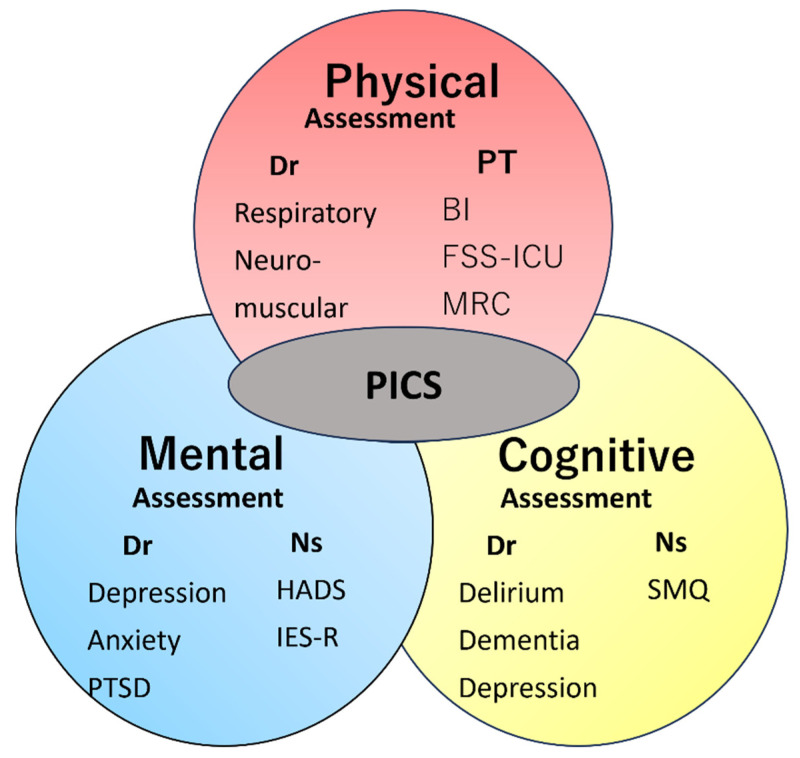
Background: Persistent inflammation, immunosuppression, and catabolism syndrome (PIICS) is known as a prolonged immunodeficiency that occurs after severe infection. Few studies have demonstrated a direct relationship between PIICS and physical dysfunction in post-intensive care syndrome (PICS). We herein investigated how each component of PICS was affected by the diagnosis of PIICS during hospitalization and examined the relationship between PIICS and PICS using PICS assessments performed at the Hitachi General Hospital PICS Clinic.
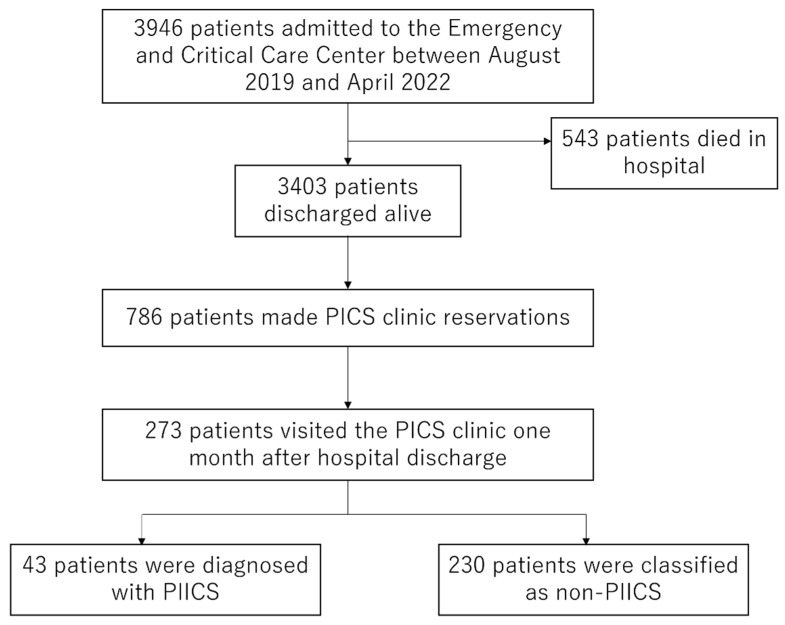
Methods: The 273 patients who visited the PICS clinic at one month after discharge from the ICU at Hitachi General Hospital were included in the study. We used the diagnostic criteria for PIICS described in previous studies. At least two of the following blood test values on day 14 of hospitalization had to be met for a diagnosis of PIICS: C-reactive protein (CRP) > 2.0 mg/dL, albumin (Alb) < 3.0 g/dL, and lymphocytes (Lym) < 800/μL. Blood test values closest to day 14 out of 11-17 days of hospitalization were used. The primary outcome was a Barthel Index (BI) < 90, while secondary outcomes were the results of various PICS assessments, including mental and cognitive impairments, performed at the PICS clinic. We supplemented missing data with multiple imputations by chained equations. We performed a nominal logistic regression analysis with age, sex, BMI, SOFA, and the presence of PIICS as variables for BI < 90.
Results: Forty-three out of two hundred seventy-three PICS outpatients met the diagnostic criteria for PIICS during hospitalization. In comparisons with non-PIICS patients, significantly higher severity scores for APACHE II and SOFA and a longer hospital stay were observed in PIICS patients, suggesting a higher clinical severity. The primary outcome, BI, was lower in the PIICS group (97.5 (58.5, 100) vs. 100 (95, 100), p = 0.008), as were the secondary outcomes (FSS-ICU: 35 (31, 35) vs. 35 (35, 35), MRC score: 55 (50.25, 58) vs. 58 (53, 60), grip strength: 16.45 (9.2, 25.47) vs. 20.4 (15.3, 27.7)). No significant differences were noted in mental or cognitive function assessments, such as HADS, IES-R, and SMQ. A multivariable analysis supplemented with missing data revealed that PIICS (odds ratio: 1.23 (1.08-1.40 p = 0.001) and age (odds ratio: 1.007 (1.004-1.01), p < 0.001) correlated with BI < 90, independent of clinical severity such as sequential organ failure assessment (SOFA). Similar results were obtained in the sensitivity analysis excluding missing data.
Conclusions: The present study revealed a strong relationship between PIICS and post-discharge PICS physical dysfunction in patients requiring intensive care.
Keywords: PICS; PICS clinic; PIICS; catabolism syndrome; critical care; immunosuppression; persistent inflammation; post-intensive care syndrome.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Disseminated Intravascular Coagulopathy Is Associated with the Outcome of Persistent Inflammation, Immunosuppression and Catabolism Syndrome.J Clin Med. 2020 Aug 17;9(8):2662. doi: 10.3390/jcm9082662. J Clin Med. 2020. PMID: 32824569 Free PMC article.
-
C-reactive protein clustering to clarify persistent inflammation, immunosuppression and catabolism syndrome.Intensive Care Med. 2020 Mar;46(3):437-443. doi: 10.1007/s00134-019-05851-3. Epub 2020 Jan 9. Intensive Care Med. 2020. PMID: 31919541
-
[Predictive value of glycosylated serum protein combined with glycemic variability on secondary persistent inflammatory immunosuppressed catabolic syndrome prediction in elderly septic patients].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2018 Nov;30(11):1051-1055. doi: 10.3760/cma.j.issn.2095-4352.2018.011.008. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2018. PMID: 30541644 Chinese.
-
Instruments to assess post-intensive care syndrome assessment: a scoping review and modified Delphi method study.Crit Care. 2023 Nov 7;27(1):430. doi: 10.1186/s13054-023-04681-6. Crit Care. 2023. PMID: 37936249 Free PMC article.
-
Persistent inflammation and immunosuppression: a common syndrome and new horizon for surgical intensive care.J Trauma Acute Care Surg. 2012 Jun;72(6):1491-501. doi: 10.1097/TA.0b013e318256e000. J Trauma Acute Care Surg. 2012. PMID: 22695412 Free PMC article. Review.
Cited by
-
Post-intensive care syndrome: Recent advances and future directions.Acute Med Surg. 2024 Feb 20;11(1):e929. doi: 10.1002/ams2.929. eCollection 2024 Jan-Dec. Acute Med Surg. 2024. PMID: 38385144 Free PMC article. Review.
-
LASSO-Based Machine Learning Algorithm for Prediction of PICS Associated with Sepsis.Infect Drug Resist. 2024 Jul 1;17:2701-2710. doi: 10.2147/IDR.S464906. eCollection 2024. Infect Drug Resist. 2024. PMID: 38974318 Free PMC article.
References
-
- Elliott D., Davidson E.J., Harvey A.M., Bemis-Dougherty A., Hopkins O.R., Iwashyna J.T., Wagner J., Weinert C., Wunsch H., Bienvenu J.O., et al. Exploring the scope of post-intensive care syndrome therapy and care: Engagement of non-critical care providers and survivors in a second stakeholders meeting. Crit. Care Med. 2014;42:2518–2526. doi: 10.1097/CCM.0000000000000525. - DOI - PubMed
-
- Mira C.J., Gentile F.L., Mathias J.B., Efron A.P., Brakenridge C.S., Mohr M.A., Moore A.F., Moldawer L.L. Sepsis pathophysiology, chronic critical illness, and persistent inflammation-immunosuppression and catabolism syndrome. Crit. Care Med. 2017;45:253–262. doi: 10.1097/CCM.0000000000002074. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
