

Digestive system deep infiltrating endometriosis: What do we know
- PMID: 37632165
- PMCID: PMC10718155
- DOI: 10.1111/jcmm.17921
Digestive system deep infiltrating endometriosis: What do we know
Abstract
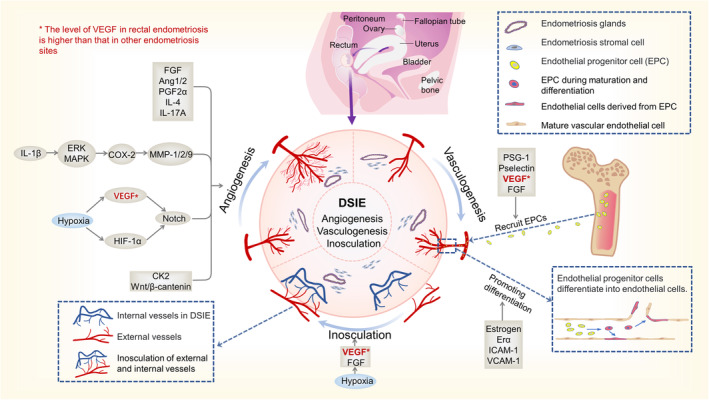
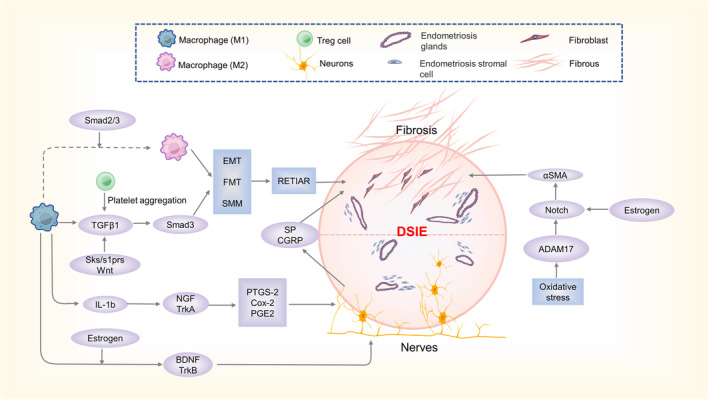
Digestive system infiltrating endometriosis (DSIE) is an uncommon form of endometriosis in the digestive system. DSIE often occurs in the intestines (especially the sigmoid rectum), liver, gallbladder and pancreas. Clinically, DSIE presents with the same symptoms as endometriosis, including cyclic pain, bleeding and infertility, in addition to specific biliary/intestinal obstruction and gastrointestinal bleeding. Compared to general endometriosis, DSIE has unique biological behaviour and pathophysiological mechanisms. Most DSIEs are deep invasive endometrioses, characterized by metastasis to the lymph nodes and lymphatic vessels, angiogenesis, peripheral nerve recruitment, fibrosis and invasion of surrounding tissues. DSIE-related peripheral angiogenesis is divided into three patterns: angiogenesis, vasculogenesis and inosculation. These patterns are regulated by interactions between multiple hypoxia-hormone cytokines. The nerve growth factors regulate the extensive neurofibril recruitment in DSIE lesions, which accounts for severe symptoms of deep pain. They are also associated with fibrosis and the aggressiveness of DSIE. Cyclic changes in DSIE lesions, recurrent inflammation and oxidative stress promote repeated tissue injury and repair (ReTIAR) mechanisms in the lesions, accelerating fibril formation and cancer-related mutations. Similar to malignant tumours, DSIE can also exhibit aggressiveness derived from collective cell migration mediated by E-cadherin and N-cadherin. This often makes DSIE misdiagnosed as a malignant tumour of the digestive system in clinical practice. In addition to surgery, novel treatments are urgently required to effectively eradicate this lesion.
Keywords: aetiology; digestive system; endometriosis; intestines; molecular mechanisms.
© 2023 The Authors. Journal of Cellular and Molecular Medicine published by Foundation for Cellular and Molecular Medicine and John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Are digestive symptoms in women presenting with pelvic endometriosis specific to lesion localizations? A preliminary prospective study.Hum Reprod. 2012 Dec;27(12):3440-9. doi: 10.1093/humrep/des322. Epub 2012 Sep 7. Hum Reprod. 2012. PMID: 22962316
-
[Intestinal endometriosis].Presse Med. 2012 Apr;41(4):358-66. doi: 10.1016/j.lpm.2011.07.017. Epub 2011 Oct 19. Presse Med. 2012. PMID: 22014564 Review. French.
-
Conservative surgery versus colorectal resection in deep endometriosis infiltrating the rectum: a randomized trial.Hum Reprod. 2018 Jan 1;33(1):47-57. doi: 10.1093/humrep/dex336. Hum Reprod. 2018. PMID: 29194531 Free PMC article. Clinical Trial.
-
Invasion of human deep nodular endometriotic lesions is associated with collective cell migration and nerve development.Fertil Steril. 2018 Dec;110(7):1318-1327. doi: 10.1016/j.fertnstert.2018.08.016. Fertil Steril. 2018. PMID: 30503131
-
Pathogenetic Mechanisms of Deep Infiltrating Endometriosis.Reprod Sci. 2015 Sep;22(9):1053-9. doi: 10.1177/1933719115592713. Epub 2015 Jul 12. Reprod Sci. 2015. PMID: 26169038 Review.
Cited by
-
The Role of NK and T Cells in Endometriosis.Int J Mol Sci. 2024 Sep 21;25(18):10141. doi: 10.3390/ijms251810141. Int J Mol Sci. 2024. PMID: 39337624 Free PMC article.
-
Intestinal endometriosis: A rare cause of acute care surgery.Ulus Travma Acil Cerrahi Derg. 2025 Jun;31(6):556-561. doi: 10.14744/tjtes.2025.85691. Ulus Travma Acil Cerrahi Derg. 2025. PMID: 40511762 Free PMC article.
References
-
- Tosti C, Pinzauti S, Santulli P, Chapron C, Petraglia F. Pathogenetic mechanisms of deep infiltrating endometriosis. Reprod Sci. 2015;22:1053‐1059. - PubMed
-
- Andres MP, Arcoverde FVL, Souza CCC, Fernandes LFC, Abrão MS, Kho RM. Extrapelvic endometriosis: a systematic review. J Minim Invasive Gynecol. 2020;27:373‐389. - PubMed
-
- Matalliotakis M, Goulielmos GN, Kalogiannidis I, Koumantakis G, Matalliotakis I, Arici A. Extra pelvic endometriosis: retrospective analysis on 200 cases in two different countries. Eur J Obstet Gynecol Reprod Biol. 2017;217:34‐37. - PubMed
-
- Yantiss RK, Clement PB, Young RH. Endometriosis of the intestinal tract: a study of 44 cases of a disease that may cause diverse challenges in clinical and pathologic evaluation. Am J Surg Pathol. 2001;25:445‐454. - PubMed
-
- Sampson JA. Peritoneal endometriosis due to the menstrual dissemination of endometrial tissue into the peritoneal cavity. Am J Obstet Gynecol. 1927;14:422‐469.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
