

Identifying molecular phenotypes in sepsis: an analysis of two prospective observational cohorts and secondary analysis of two randomised controlled trials
- PMID: 37633303
- PMCID: PMC10841178
- DOI: 10.1016/S2213-2600(23)00237-0
Identifying molecular phenotypes in sepsis: an analysis of two prospective observational cohorts and secondary analysis of two randomised controlled trials
Abstract
Background: In sepsis and acute respiratory distress syndrome (ARDS), heterogeneity has contributed to difficulty identifying effective pharmacotherapies. In ARDS, two molecular phenotypes (hypoinflammatory and hyperinflammatory) have consistently been identified, with divergent outcomes and treatment responses. In this study, we sought to derive molecular phenotypes in critically ill adults with sepsis, determine their overlap with previous ARDS phenotypes, and evaluate whether they respond differently to treatment in completed sepsis trials.
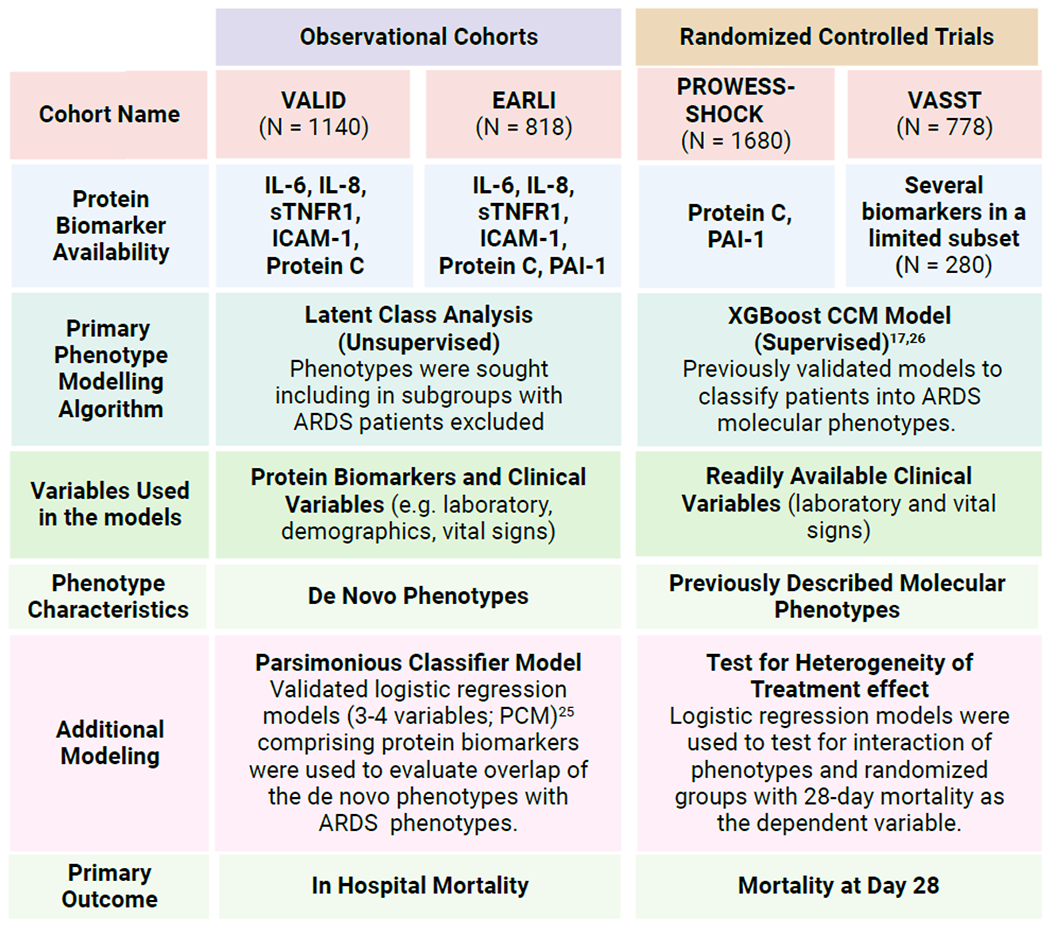
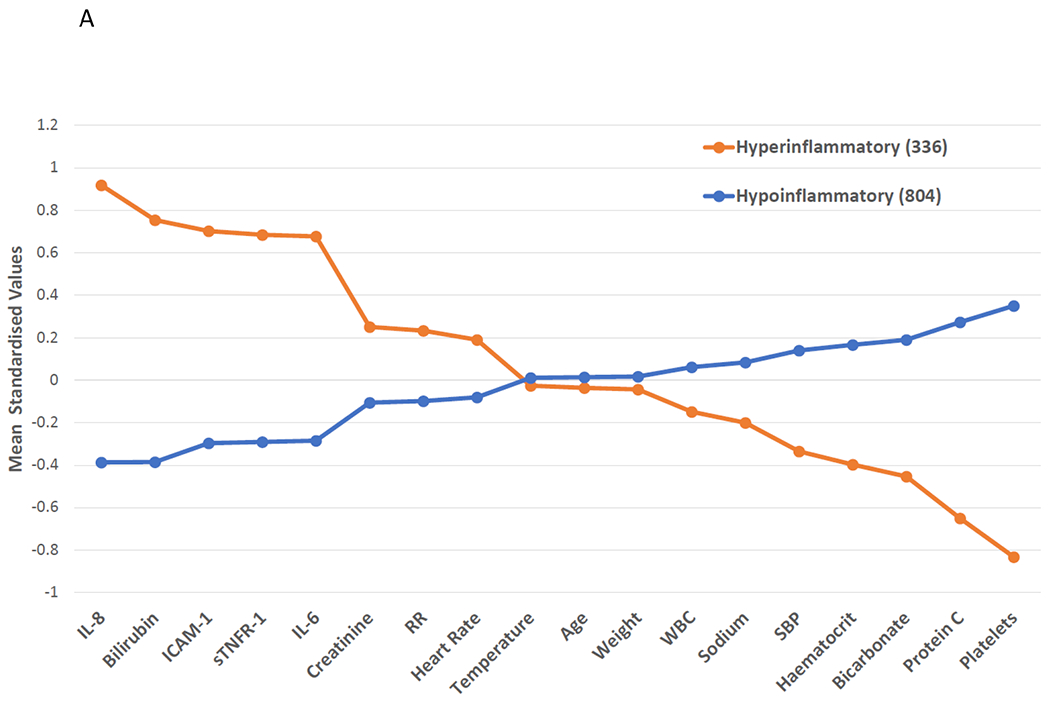
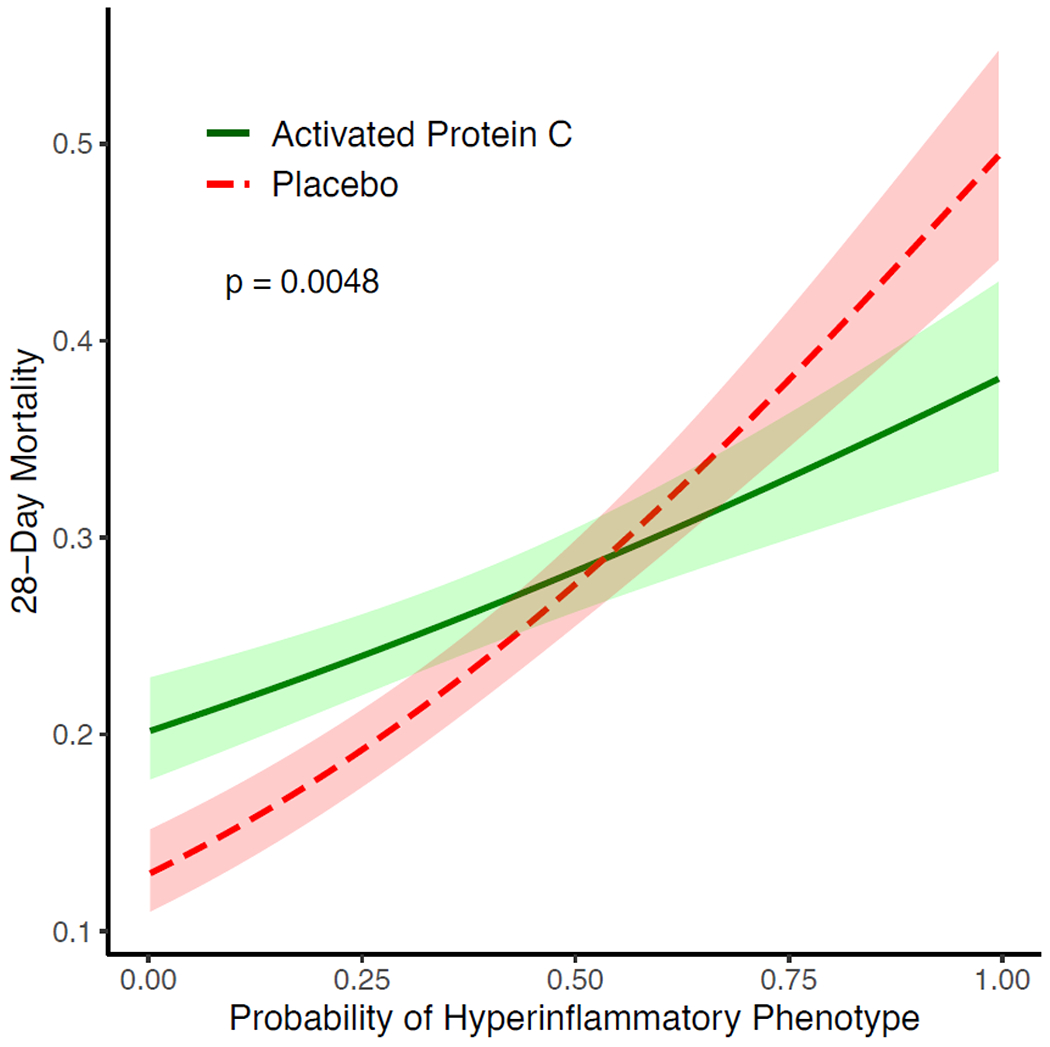
Methods: We used clinical data and plasma biomarkers from two prospective sepsis cohorts, the Validating Acute Lung Injury biomarkers for Diagnosis (VALID) study (N=1140) and the Early Assessment of Renal and Lung Injury (EARLI) study (N=818), in latent class analysis (LCA) to identify the optimal number of classes in each cohort independently. We used validated models trained to classify ARDS phenotypes to evaluate concordance of sepsis and ARDS phenotypes. We applied these models retrospectively to the previously published Prospective Recombinant Human Activated Protein C Worldwide Evaluation in Severe Sepsis and Septic Shock (PROWESS-SHOCK) trial and Vasopressin and Septic Shock Trial (VASST) to assign phenotypes and evaluate heterogeneity of treatment effect.
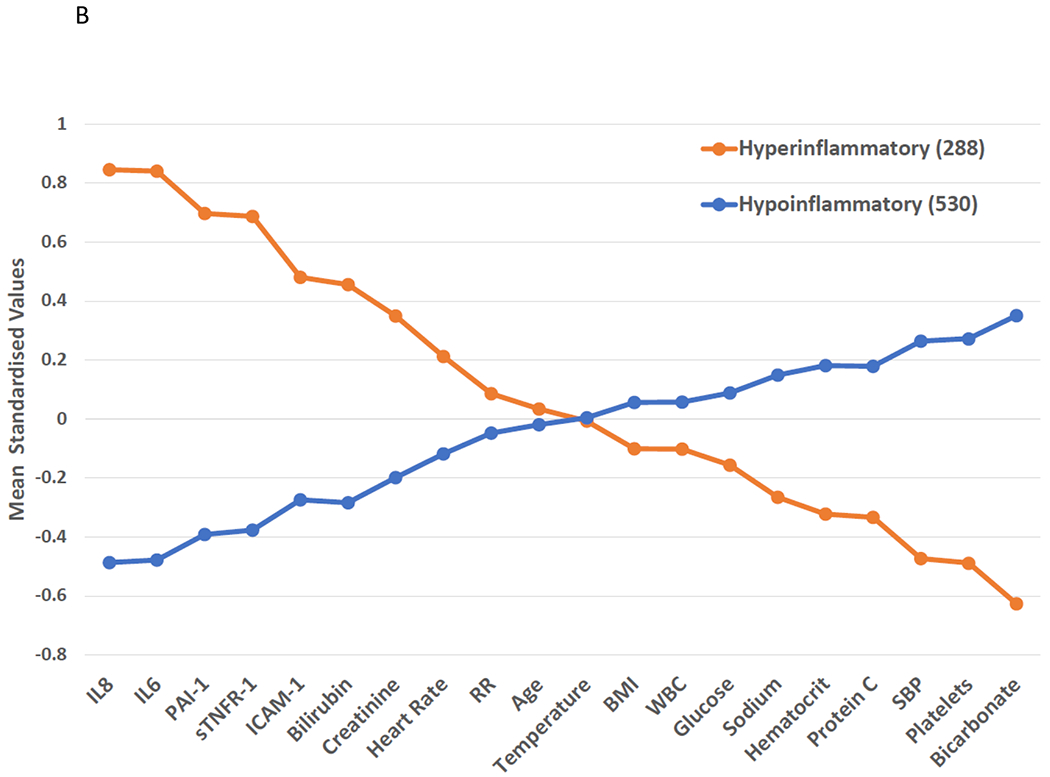
Findings: A two-class model best fit both VALID and EARLI (p<0·0001). In VALID, 804 (70·5%) of the 1140 patients were classified as hypoinflammatory and 336 (29·5%) as hyperinflammatory; in EARLI, 530 (64·8%) of 818 were hypoinflammatory and 288 (35·2%) hyperinflammatory. We observed higher plasma pro-inflammatory cytokines, more vasopressor use, more bacteraemia, lower protein C, and higher mortality in the hyperinflammatory than in the hypoinflammatory phenotype (p<0·0001 for all). Classifier models indicated strong concordance between sepsis phenotypes and previously identified ARDS phenotypes (area under the curve 0·87-0·96, depending on the model). Findings were similar excluding participants with both sepsis and ARDS. In PROWESS-SHOCK, 1142 (68·0%) of 1680 patients had the hypoinflammatory phenotype and 538 (32·0%) had the hyperinflammatory phenotype, and response to activated protein C differed by phenotype (p=0·0043). In VASST, phenotype proportions were similar to other cohorts; however, no treatment interaction with the type of vasopressor was observed (p=0·72).
Interpretation: Molecular phenotypes previously identified in ARDS are also identifiable in multiple sepsis cohorts and respond differently to activated protein C. Molecular phenotypes could represent a treatable trait in critical illness beyond the patient's syndromic diagnosis.
Funding: US National Institutes of Health.
Copyright © 2023 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests PS reports funding from the US National Institutes of Health (NIH) and National Institute of General Medical Sciences; and consulting fees from AstraZeneca. LBW reports funding from NIH, Department of Defense (DoD), Genentech, Boehringer Ingelheim, and CSL Behring; consulting fees from Akebia Therapeutics, Santhera, Global Blood Therapeutics, and Boehringer Ingelheim; and stock options in Virtuoso Surgical. CSC reports funding from NIH; research grants from Roche Genentech and Quantum Leap Healthcare Collaborative; consulting fees from Vasomune Therapeutics, GEn1E Lifesciences, NGM Bio, Cellenkos, and Janssen; and a patent on metagenomic sequencing for sepsis diagnosis (co-recipient). MAM reports funding from Roche Genentech, Quantum Therapeutics, NIH/National Heart, Lung, and Blood Institute/National Institute of Allergy and Infectious Diseases, DoD, and California Institute for Regenerative Medicine; and consulting fees from Johnson & Johnson, Gilead Sciences, and Novartis. MMC reports funding from NIH and DoD; and intellectual property royalties from an issued patent (#11 410 777). JAR reports an investigator-initiated grant from Grifols provided to and administered by the University of British Columbia, Canadian Institutes of Health Research; three grants from the St Paul's Foundation; patents owned by the University of British Columbia related to the use of PCSK9 inhibitor(s) in sepsis and the use of vasopressin in septic shock, and by Ferring Pharmaceuticals for use of selepressin in septic shock; formerly being a founder, Director, and shareholder in Cyon Therapeutics (now closed); being a shareholder in Molecular You; receiving consulting fees in the last 3 years from SIB, Ferring Pharmaceuticals, and Par Pharmaceutical; and having been a funded member of the Data and Safety Monitoring Board of an NIH-sponsored trial of plasma in COVID-19 (PASS-IT-ON). KDL reports grants from NIH: National Institute of Diabetes and Digestive and Kidney Diseases; consulting fees from bioMérieux, UpToDate, SeaStar Medical, AM-Pharma, and Baxter; and stock or stock options in Amgen. All other authors declare no competing interests.
Figures
Comment in
-
Beyond patterns: how to assign biological meaning to ARDS and sepsis phenotypes.Lancet Respir Med. 2023 Nov;11(11):946-947. doi: 10.1016/S2213-2600(23)00266-7. Epub 2023 Aug 23. Lancet Respir Med. 2023. PMID: 37633305 No abstract available.
References
-
- Marshall JC. Why have clinical trials in sepsis failed? Trends Mol Med. 2014;20(4):195–203. - PubMed
-
- Matthay MA, McAuley DF, Ware LB. Clinical trials in acute respiratory distress syndrome: challenges and opportunities. Lancet Respir Med. 2017;5(6):524–34. - PubMed
-
- Corren J, Lemanske RF, Hanania NA, Korenblat PE, Parsey MV, Arron JR, et al. Lebrikizumab treatment in adults with asthma. N Engl J Med. 2011;365(12):1088–98. - PubMed
-
- Romond EH, Perez EA, Bryant J, Suman VJ, Geyer CE Jr., Davidson NE, et al. Trastuzumab plus adjuvant chemotherapy for operable HER2-positive breast cancer. N Engl J Med. 2005;353(16):1673–84. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
