

Uterus-preserving surgical management of placenta accreta spectrum disorder: a large retrospective study
- PMID: 37633887
- PMCID: PMC10464453
- DOI: 10.1186/s12884-023-05923-9
Uterus-preserving surgical management of placenta accreta spectrum disorder: a large retrospective study
Abstract
Background: The two-child policy implemented in China resulted in a surge of high-risk pregnancies among advanced maternal aged women and presented a window of opportunity to identify a large number of placenta accreta spectrum (PAS) cases, which often invoke severe blood loss and hysterectomy. We thus had an opportunity to evaluate the surgical outcomes of a unique conservative PAS management strategy for uterus preservation, and the impacts of magnetic resonance imaging (MRI) in PAS surgical planning.
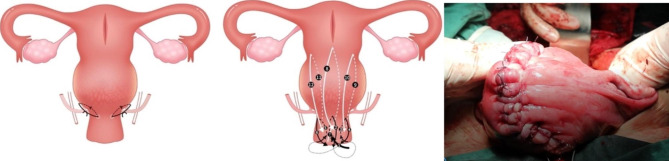
Methods: Cross-sectional study, comparing the outcomes of a new uterine artery ligation combined with clover suturing technique (UAL + CST) with the existing conservative surgical approaches in a maternal public hospital with an annual birth of more than 20,000 neonates among all placenta previa cases suspecting of PAS between January 1, 2015 and December 31, 2018.
Results: From a total of 89,397 live births, we identified 210 PAS cases from 400 singleton pregnancies with placenta previa. Aside from 2 self-requested natural births (low-lying placenta), all PAS cases had safe cesarean deliveries without any total hysterectomy. Compared with the existing approaches, the evaluated UAL + CST had a significant reduction in intraoperative blood loss (β=-312 ml, P < .001), RBC transfusion (β=-1.08 unit, P = .001), but required more surgery time (β = 16.43 min, P = .01). MRI-measured placenta thickness, when above 50 mm, can increase blood loss (β = 315 ml, P = .01), RBC transfusion (β = 1.28 unit, P = .01), surgery time (β = 48.84 min, P < .001) and hospital stay (β = 2.58 day, P < .001). A majority of percreta patients resumed normal menstrual cycle within 12 months with normal menstrual fluid volume, without abnormal urination or defecation.
Conclusions: A conservative surgical management approach of UAL + CST for PAS is safe and effective with a low complication rate. MRI might be useful for planning PAS surgery.
Clinical trial registration number: ChiCTR2000035202.
Keywords: Conservative management; Placenta accreta spectrum; Placenta previa; Uterus preservation.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Bowman ZS, Eller AG, Bardsley TR, Greene T, Varner MW, Silver RM. Risk factors for placenta accreta: a large prospective cohort. Am J Perinatol. 2014;31(9):799–804. - PubMed
Publication types
MeSH terms
Grants and funding
- grant number Y2021MS08/Linyi Maternal and Child Healthcare Hospital
- grant number Y2021MS08/Linyi Maternal and Child Healthcare Hospital
- grant number Y2021MS08/Linyi Maternal and Child Healthcare Hospital
- grant number Y2021MS08/Linyi Maternal and Child Healthcare Hospital
- grant number Y2021MS08/Linyi Maternal and Child Healthcare Hospital
- grant number Y2021MS08/Linyi Maternal and Child Healthcare Hospital
- grant number Y2021MS08/Linyi Maternal and Child Healthcare Hospital
- grant number Y2021MS08/Linyi Maternal and Child Healthcare Hospital
- grant number Y2021MS08/Linyi Maternal and Child Healthcare Hospital
- grant number Y2021MS08/Linyi Maternal and Child Healthcare Hospital
- grant number Y2021MS08/Linyi Maternal and Child Healthcare Hospital
LinkOut - more resources
Full Text Sources
