

Haloperidol for the treatment of delirium in critically ill patients: an updated systematic review with meta-analysis and trial sequential analysis
- PMID: 37633991
- PMCID: PMC10463604
- DOI: 10.1186/s13054-023-04621-4
Haloperidol for the treatment of delirium in critically ill patients: an updated systematic review with meta-analysis and trial sequential analysis
Abstract
Background: Haloperidol is frequently used in critically ill patients with delirium, but evidence for its effects has been sparse and inconclusive. By including recent trials, we updated a systematic review assessing effects of haloperidol on mortality and serious adverse events in critically ill patients with delirium.
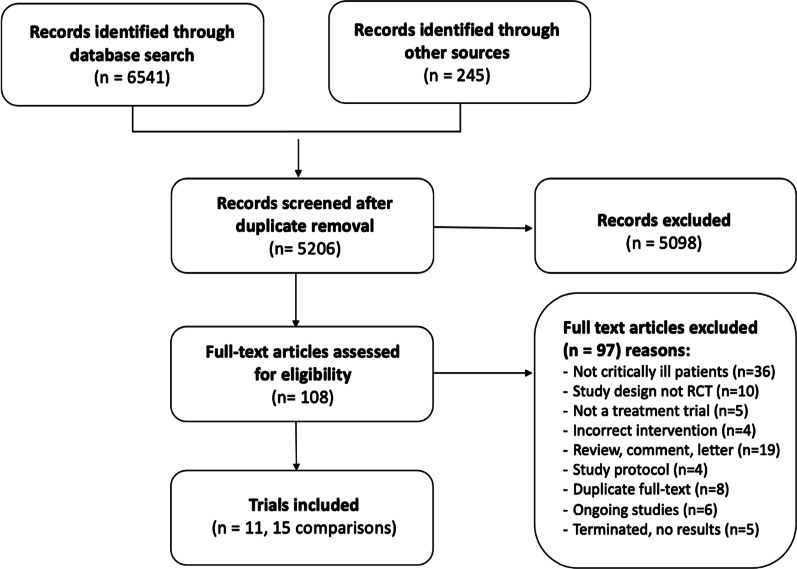
Methods: This is an updated systematic review with meta-analysis and trial sequential analysis of randomised clinical trials investigating haloperidol versus placebo or any comparator in critically ill patients with delirium. We adhered to the Cochrane handbook, the PRISMA guidelines and the grading of recommendations assessment, development and evaluation statements. The primary outcomes were all-cause mortality and proportion of patients with one or more serious adverse events or reactions (SAEs/SARs). Secondary outcomes were days alive without delirium or coma, delirium severity, cognitive function and health-related quality of life.
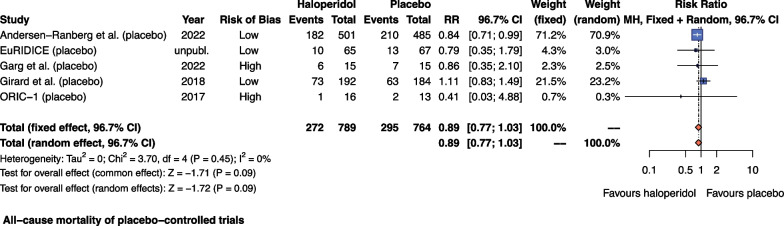
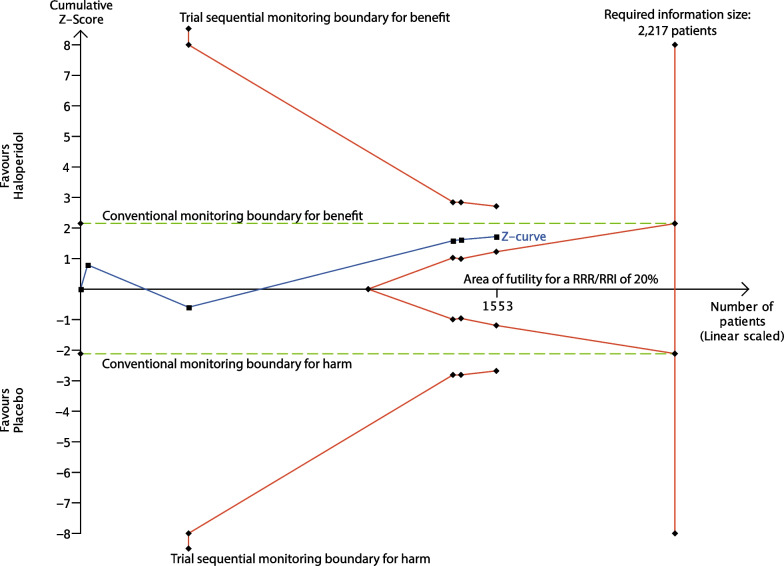
Results: We included 11 RCTs with 15 comparisons (n = 2200); five were placebo-controlled. The relative risk for mortality with haloperidol versus placebo was 0.89; 96.7% CI 0.77 to 1.03; I2 = 0% (moderate-certainty evidence) and for proportion of patients experiencing SAEs/SARs 0.94; 96.7% CI 0.81 to 1.10; I2 = 18% (low-certainty evidence). We found no difference in days alive without delirium or coma (moderate-certainty evidence). We found sparse data for other secondary outcomes and other comparators than placebo.
Conclusions: Haloperidol may reduce mortality and likely result in little to no change in the occurrence of SAEs/SARs compared with placebo in critically ill patients with delirium. However, the results were not statistically significant and more trial data are needed to provide higher certainty for the effects of haloperidol in these patients.
Trial registration: CRD42017081133, date of registration 28 November 2017.
Keywords: Antipsychotics; Delirium; Haloperidol; Meta-analysis; Systematic review.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
NCAN was the coordinating investigator of the AID-ICU trial. NCAN, OMAT, AP, LMP and JW were part of the steering committee of the AID-ICU trial. JW has been a member of the task force to develop theory and software for TSA at Copenhagen Trial Unit. MOC was primary investigator of the AID-ICU cohort study. MvdJ and LS are the Principal Investigator and Coordinating Investigator of the EuRIDICE trial. AP has received honorarium for advisory board work with Novartis. MM and MB have nothing to declare.
Figures
References
-
- Association AP. Diagnostic and statistical manual of mental disorders, Fifth edition. American Psychiatric Association; 2013. p. 991.
-
- Krewulak KD, et al. Incidence and prevalence of delirium subtypes in an adult ICU: a systematic review and meta-analysis. Crit Care Med. 2018;46(12):2029–2035. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
