

Semaglutide in HFpEF across obesity class and by body weight reduction: a prespecified analysis of the STEP-HFpEF trial
- PMID: 37635157
- PMCID: PMC10504076
- DOI: 10.1038/s41591-023-02526-x
Semaglutide in HFpEF across obesity class and by body weight reduction: a prespecified analysis of the STEP-HFpEF trial
Abstract
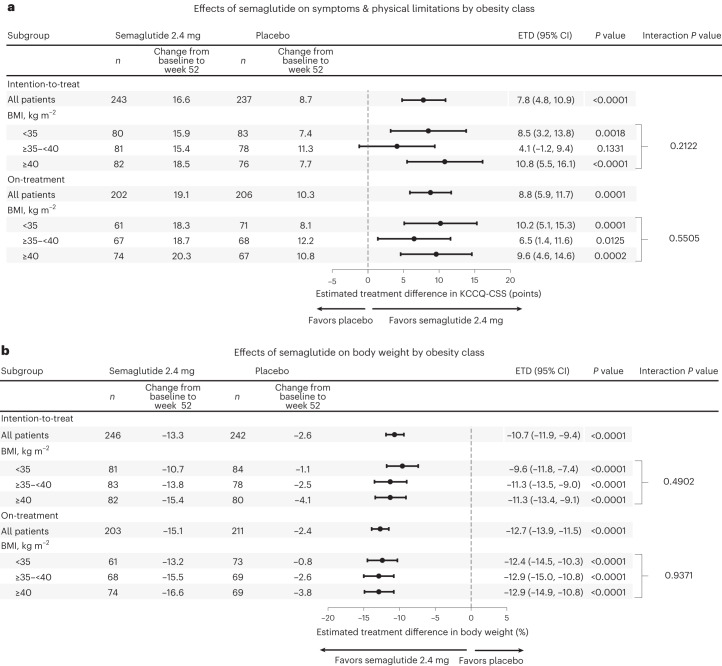
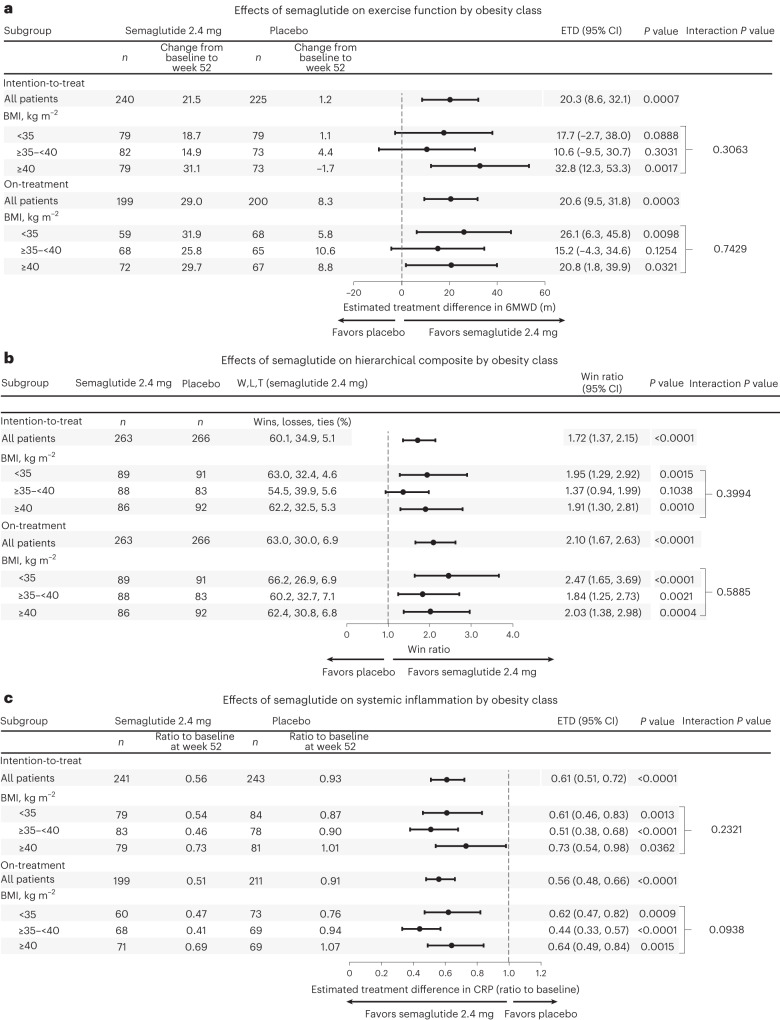
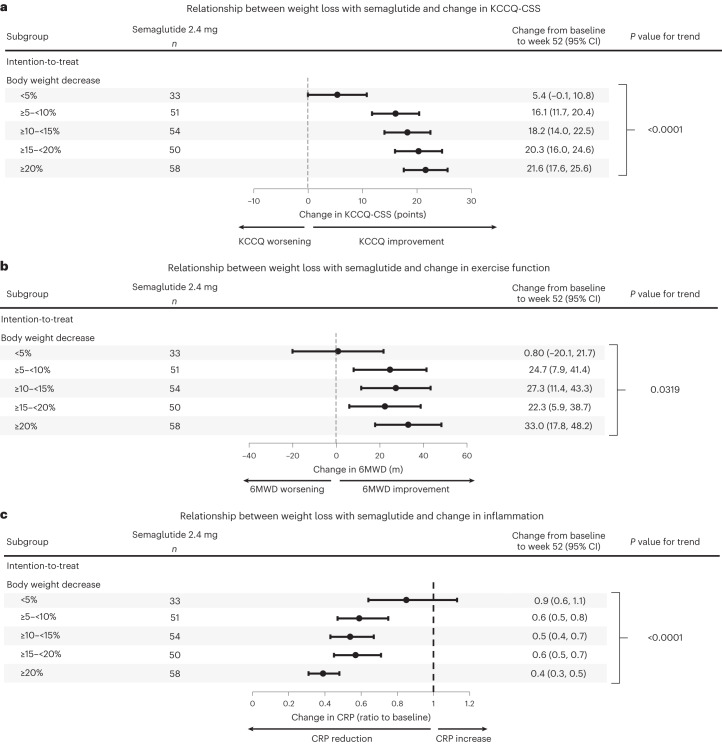
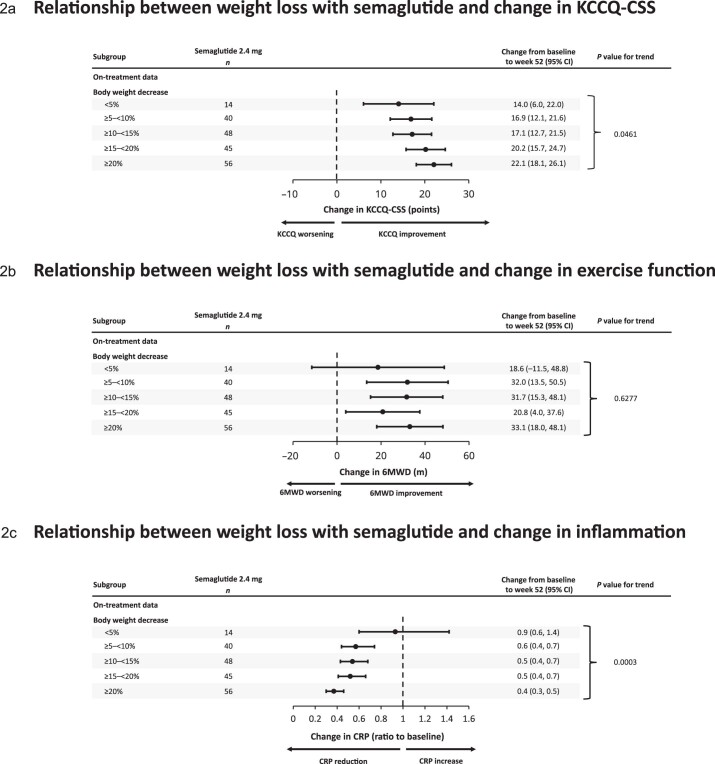
In the STEP-HFpEF trial, semaglutide improved symptoms, physical limitations and exercise function and reduced body weight in patients with obesity phenotype of heart failure and preserved ejection fraction (HFpEF). This prespecified analysis examined the effects of semaglutide on dual primary endpoints (change in Kansas City Cardiomyopathy Questionnaire-Clinical Summary Score (KCCQ-CSS) and body weight) and confirmatory secondary endpoints (change in 6-minute walk distance (6MWD), hierarchical composite (death, HF events, change in KCCQ-CSS and 6MWD) and change in C-reactive protein (CRP)) across obesity classes I-III (body mass index (BMI) 30.0-34.9 kg m-2, 35.0-39.9 kg m-2 and ≥40 kg m-2) and according to body weight reduction with semaglutide after 52 weeks. Semaglutide consistently improved all outcomes across obesity categories (P value for treatment effects × BMI interactions = not significant for all). In semaglutide-treated patients, improvements in KCCQ-CSS, 6MWD and CRP were greater with larger body weight reduction (for example, 6.4-point (95% confidence interval (CI): 4.1, 8.8) and 14.4-m (95% CI: 5.5, 23.3) improvements in KCCQ-CSS and 6MWD for each 10% body weight reduction). In participants with obesity phenotype of HFpEF, semaglutide improved symptoms, physical limitations and exercise function and reduced inflammation and body weight across obesity categories. In semaglutide-treated patients, the magnitude of benefit was directly related to the extent of weight loss. Collectively, these data support semaglutide-mediated weight loss as a key treatment strategy in patients with obesity phenotype of HFpEF. ClinicalTrials.gov identifier: NCT04788511 .
© 2023. The Author(s).
Conflict of interest statement
B.A.B. receives research support from the National Institutes of Health (NIH) and the US Department of Defense as well as research grant funding from AstraZeneca, Axon, GlaxoSmithKline, Medtronic, Mesoblast, Novo Nordisk, Rivus and Tenax Therapeutics. B.A.B. has also served as a consultant for Actelion, Amgen, Aria, Axon Therapies, BD Biosciences, Boehringer Ingelheim, Cytokinetics, Edwards Lifesciences, Eli Lilly, Imbria, Janssen, Merck, Novo Nordisk, NGM Biopharmaceuticals, NXT and VADovations and is named as an inventor (US patent no. 10,307,179) for the tools and approach for a minimally invasive pericardial modification procedure to treat heart failure. D.W.K. was supported, in part, by the Kermit Glenn Phillips II Chair in Cardiovascular Medicine and NIH grants U01AG076928, R01AG078153, R01AG045551, R01AG18915 and U01HL160272 and reports receiving honoraria as a consultant for Bayer, Corvia Medical, Boehringer Ingelheim, Ketyo, Rivus, Novo Nordisk, AstraZeneca, Pfizer and Novartis; grant funding from Novartis, Bayer, Novo Nordisk, Rivus, Pfizer and AstraZeneca; and stock ownership in Gilead Sciences. M.J.D. has acted as a consultant, advisory board member and speaker for Boehringer Ingelheim, Eli Lilly, Novo Nordisk and Sanofi; an advisory board member and speaker for AstraZeneca; an advisory board member for Pfizer, Medtronic and ShouTi Pharma Inc.; and a speaker for Novartis, Sanofi and Amgen. M.D. has received grants in support of investigator and investigator-initiated trials from AstraZeneca, Sanofi-Aventis, Eli Lilly, Boehringer Ingelheim, Janssen and Novo Nordisk. J.B. is a consultant to Abbott, American Regent, Amgen, Applied Therapeutic, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol Myers Squibb, Cardiac Dimension, Cardior, CVRx, Cytokinetics, Edwards, Element Science, Innolife, Impulse Dynamics, Imbria, Inventiva, Lexicon, Eli Lilly, LivaNova, Janssen, Medtronics, Merck, Occlutech, Novartis, Novo Nordisk, Pfizer, Pharmacosmos, Pharmain, Roche, Sequana, SQ Innovation, 3live and Vifor. M.C.P. has received research grants or consultancy fees from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Napp Pharmaceuticals, Novartis, Novo Nordisk, Pharmacosmos, Roche and SQ Innovations; has served on committees for AbbVie, Akero, Alnylam, AstraZeneca, Bayer, Boehringer Ingelheim, GlaxoSmithKline, New Amsterdam, Novo Nordisk, Resverlogix and Teikoku; and is Director of Global Clinical Trial Partners. S.J.S. reports receiving consulting fees from Abbott, AstraZeneca, Amgen, Aria CV, Axon Therapies, Bayer, Boehringer Ingelheim, Boston Scientific, Bristol Myers Squibb, Cyclerion, Cytokinetics, Edwards Lifesciences, Eidos, Imara, Impulse Dynamics, Intellia, Ionis, Eli Lilly, Merck, Metabolic Flux, MyoKardia, NGM Biopharmaceuticals, Novartis, Novo Nordisk, Pfizer, Prothena, Regeneron, Rivus, Sardocor, Shifamed, Tenax, Tenaya and United Therapeutics. S.V. reports speaking honoraria and/or consulting fees from Abbott, AstraZeneca, Bayer, Boehringer Ingelheim, Novo Nordisk, Novartis, Merck, PhaseBio, HLS Therapeutics, Amarin, Eli Lilly, Janssen, Pfizer, TIMI, Canadian Medical and Surgical Knowledge Translation Research Group. W.A. reports honoraria and/or consulting fees from Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Novartis and Novo Nordisk. F.Z.A. reports honoraria and/or consulting fees from Abbott, AstraZeneca, Medtronic, Novo Nordisk, Occlutech, Pharmacosmos and Vifor. V.C. reports speaker fees from AstraZeneca, Boehringer Ingelheim, Cipla, Dr. Reddy’s, Lupin, Novartis, Novo Nordisk, Mankind, Pfizer, Sanofi, Sun Pharma and Torrent. J.E. reports research support for trial leadership from American Regent, Applied Therapeutics, Bayer, Cytokinetics, Merck and Novo Nordisk; honoraria for consultancy from AstraZeneca, Bayer, Boehringer Ingelheim, Novartis, Novo Nordisk and Otsuka; and service as an advisor to US2.ai. M.F. reports no conflicts of interest. H.I. reports honoraria and/or consulting fees from AstraZeneca, Bayer, Boehringer Ingelheim, Daiichi-Sankyo, Mochida, Novartis and Novo Nordisk. M.L. reports honoraria and/or consulting fees from AstraZeneca, Bayer, Boehringer Ingelheim, Ewopharma, Gedeon Richter, Novartis, Novo Nordisk, Roche and Servier. V.M. reports consulting fees from Bayer, Merck Sharp & Dohme and Novo Nordisk; research grants from Regeneron; and research support from the National Institute for Research of Metabolic and Cardiovascular Diseases (Program EXCELES, project no. LX22NPO5104), funded by the European Union–Next Generation EU. J.N. reports honoraria and/or consulting fees from Alleviant, AstraZeneca, Bayer, Boehringer Ingelheim, Cytokinetics, Pfizer, Novartis, Novo Nordisk, Rovi and Vifor. E.P. reports honoraria from Novo Nordisk. M. Schou reports speaker fees from AstraZeneca, Boehringer Ingelheim, Novartis and Novo Nordisk. M. Senni reports honoraria and/or consulting fees from Abbott, AstraZeneca, Bayer, Boehringer Ingelheim, Merck, Merck Sharp & Dohme, Novartis, Novo Nordisk and Vifor. P.v.d.M. reports institutional payments for consultancy fees and/or grants from AstraZeneca, Boehringer Ingelheim, BridgeBio, Ionis, Novartis, Novo Nordisk, Pfizer, Pharmacosmoc, Pharma Nord and Vifor. D.V.L. reports honoraria and/or consulting fees from AstraZeneca, Bayer, Boehringer Ingelheim, Merck Sharp & Dohme, Novartis, Novo Nordisk, Recardio, Sanofi, Sanova and Vaxxinity. D.W. reports consultancy fees from Novo Nordisk. S.R., E.B., M.N.E., G.K.H. and D.V.M. are employees of and hold shares in Novo Nordisk A/S. M.N.K. served as a consultant or on an advisory board for 35Pharma, Alnylam, Amgen, Applied Therapeutics, AstraZeneca, Bayer, Boehringer Ingelheim, Cytokinetics, Dexcom, Eli Lilly, Esperion Therapeutics, Janssen, Lexicon Pharmaceuticals, Merck (Diabetes and Cardiovascular), Novo Nordisk, Pharmacosmos, Pfizer, scPharmaceuticals, Sanofi, Structure Therapeutics, Vifor and Youngene Therapeutics. M.N.K. has also received research grants from AstraZeneca, Boehringer Ingelheim and Pfizer; holds stock in Artera Health and Saghmos Therapeutics; has received honoraria from AstraZeneca, Boehringer Ingelheim and Novo Nordisk; and has received other research support from AstraZeneca.
Figures
Comment in
-
Body weight reduction by semaglutide administration has beneficial effect in obesity phenotype HFpEF.Nat Cardiovasc Res. 2023 Oct;2(10):858. doi: 10.1038/s44161-023-00353-4. Nat Cardiovasc Res. 2023. PMID: 39196255 No abstract available.
References
-
- Morgen, C. S. et al. Obesity, cardiorenal comorbidities and risk of hospitalization in patients with heart failure with preserved ejection fraction. Mayo Clin. Proc. 10.1016/j.mayocp.2023.07.008 (2023). - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- R01 HL162828/HL/NHLBI NIH HHS/United States
- R01 AG078153/AG/NIA NIH HHS/United States
- R01 HL140731/HL/NHLBI NIH HHS/United States
- R01 HL128526/HL/NHLBI NIH HHS/United States
- R01 HL127028/HL/NHLBI NIH HHS/United States
- R01 AG018915/AG/NIA NIH HHS/United States
- U24 AG059624/AG/NIA NIH HHS/United States
- R01 HL107577/HL/NHLBI NIH HHS/United States
- R01 HL149423/HL/NHLBI NIH HHS/United States
- P30 AG021332/AG/NIA NIH HHS/United States
- UL1 TR002384/TR/NCATS NIH HHS/United States
- R01 AG045551/AG/NIA NIH HHS/United States
- U54 HL160273/HL/NHLBI NIH HHS/United States
- U01 HL160272/HL/NHLBI NIH HHS/United States
- U01 HL160226/HL/NHLBI NIH HHS/United States
- U01 AG076928/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
