

Immune checkpoint therapy for solid tumours: clinical dilemmas and future trends
- PMID: 37635168
- PMCID: PMC10460796
- DOI: 10.1038/s41392-023-01522-4
Immune checkpoint therapy for solid tumours: clinical dilemmas and future trends
Abstract
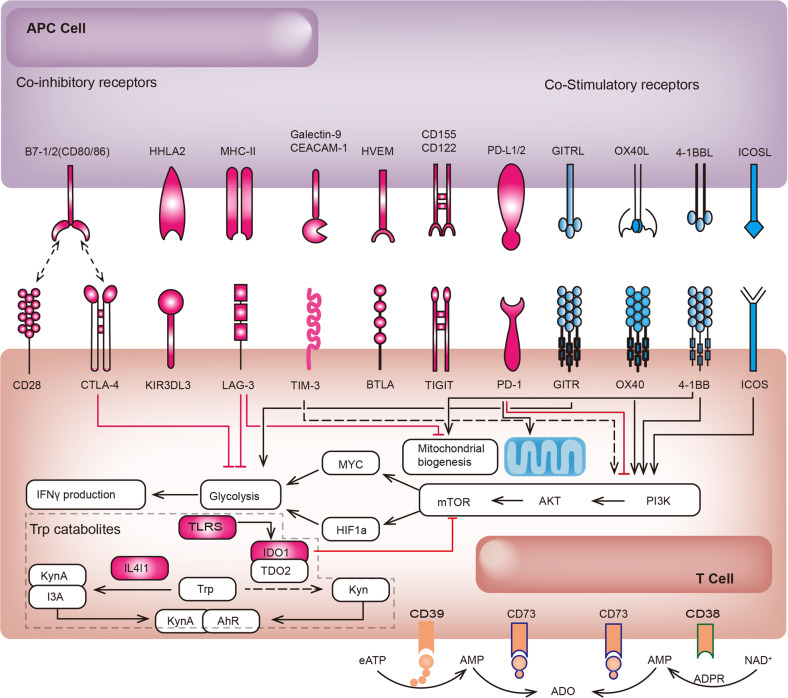
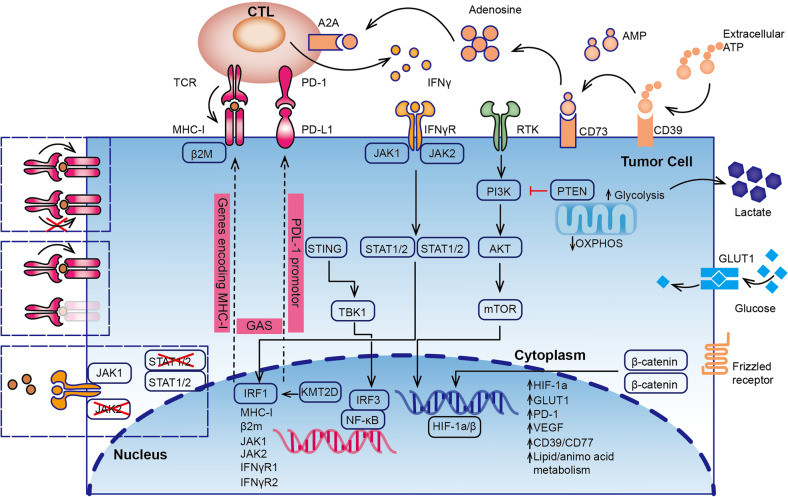
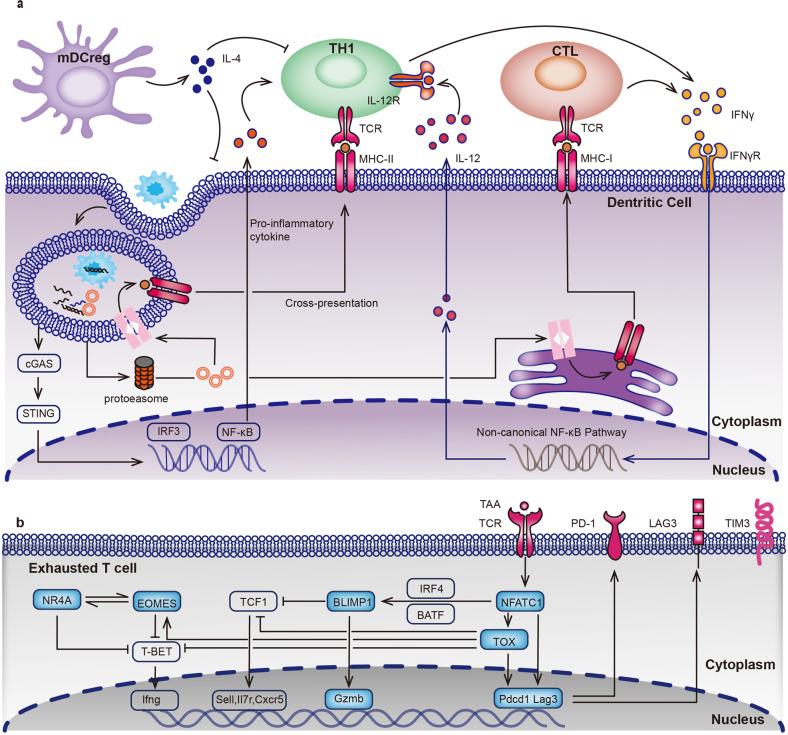
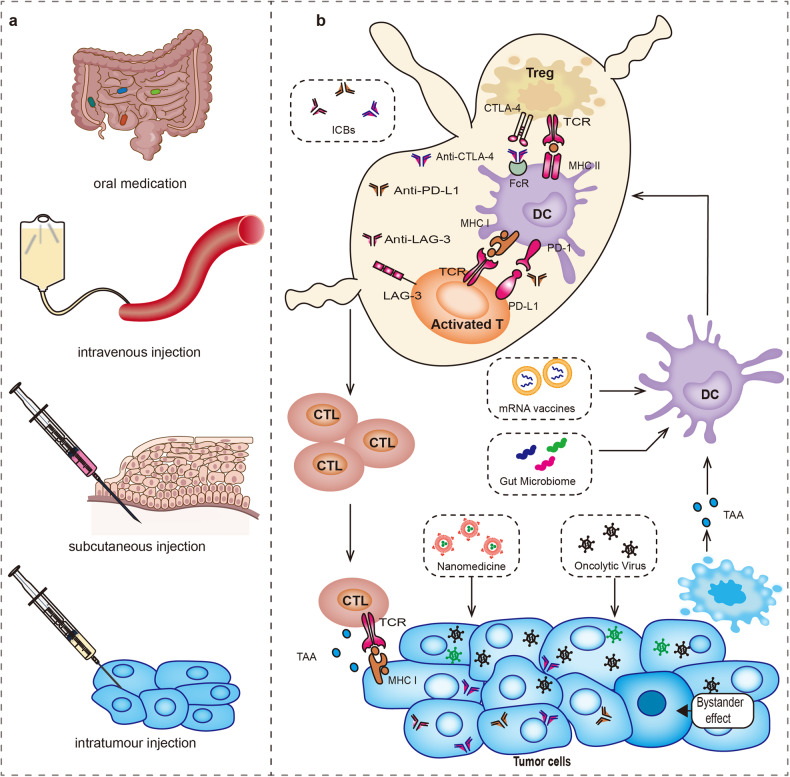
Immune-checkpoint inhibitors (ICBs), in addition to targeting CTLA-4, PD-1, and PD-L1, novel targeting LAG-3 drugs have also been approved in clinical application. With the widespread use of the drug, we must deeply analyze the dilemma of the agents and seek a breakthrough in the treatment prospect. Over the past decades, these agents have demonstrated dramatic efficacy, especially in patients with melanoma and non-small cell lung cancer (NSCLC). Nonetheless, in the field of a broad concept of solid tumours, non-specific indications, inseparable immune response and side effects, unconfirmed progressive disease, and complex regulatory networks of immune resistance are four barriers that limit its widespread application. Fortunately, the successful clinical trials of novel ICB agents and combination therapies, the advent of the era of oncolytic virus gene editing, and the breakthrough of the technical barriers of mRNA vaccines and nano-delivery systems have made remarkable breakthroughs currently. In this review, we enumerate the mechanisms of each immune checkpoint targets, associations between ICB with tumour mutation burden, key immune regulatory or resistance signalling pathways, the specific clinical evidence of the efficacy of classical targets and new targets among different tumour types and put forward dialectical thoughts on drug safety. Finally, we discuss the importance of accurate triage of ICB based on recent advances in predictive biomarkers and diagnostic testing techniques.
© 2023. West China Hospital, Sichuan University.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
