

The Impact of Unilateral 90Y-radioembolization on Functional Changes in the Contralateral Hepatic Lobe: The Prospective, Open-label RadioEmbolization, Volumetry, and Liver FuncTion Measurements (REVoluTion) Study
- PMID: 37635822
- PMCID: PMC10455191
- DOI: 10.1097/AS9.0000000000000095
The Impact of Unilateral 90Y-radioembolization on Functional Changes in the Contralateral Hepatic Lobe: The Prospective, Open-label RadioEmbolization, Volumetry, and Liver FuncTion Measurements (REVoluTion) Study
Abstract
Objectives: To investigate how metabolic function of the contralateral liver lobe is affected by unilateral radioembolization (RE), and to compare the changes in volume and metabolic function.
Background: Unilateral RE induces contralateral liver hypertrophy, but it is unknown if metabolic liver function improves in line with volume increases.
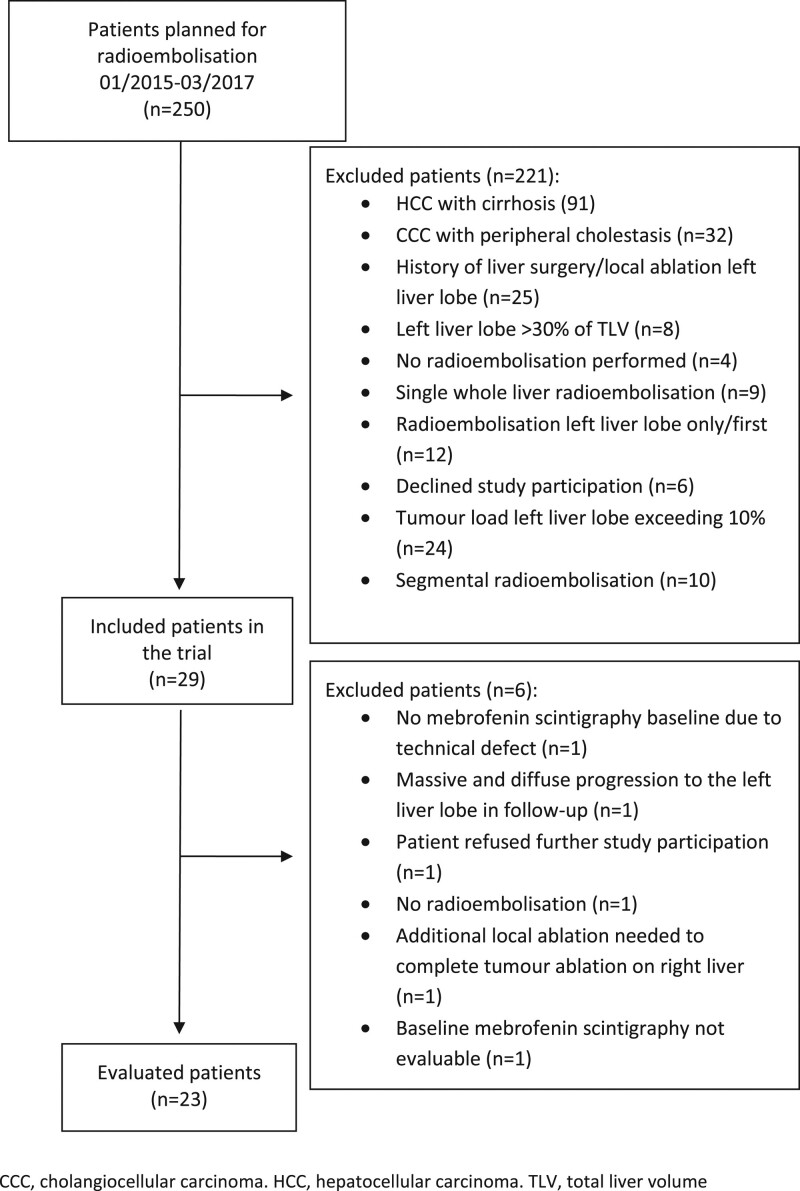
Methods: This prospective open-label, nonrandomized, therapy-optimizing study included all consecutive patients undergoing right-sided or sequential 90Y-RE for liver malignancies without underlying liver disease or biliary obstruction at a single center in Germany. Magnetic resonance imaging volumetry and hepatobiliary scintigraphy were performed immediately before RE and approximately 6 weeks after RE.
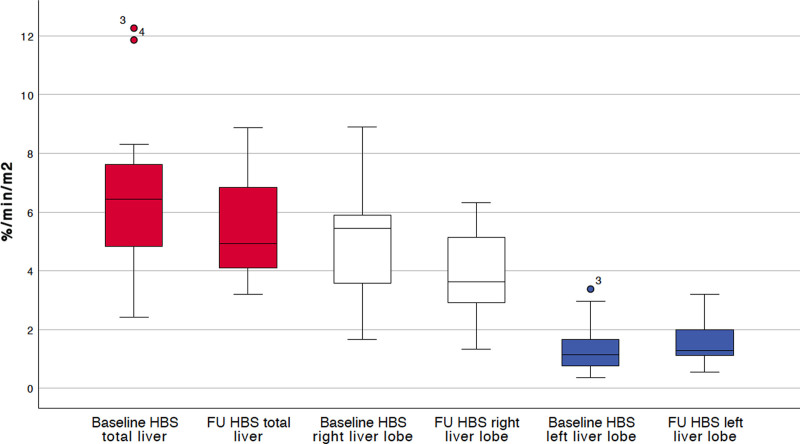
Results: Twenty-three patients were evaluated (11 metastatic colorectal cancer, 4 cholangiocellular carcinoma, 3 metastatic breast cancer, 1 each of metastatic neuroendocrine tumor, hepatocellular carcinoma, renal cell carcinoma, oesophageal cancer, pancreatic ductal adenocarcinoma). In the untreated contralateral left liver lobe, mean (SD) metabolic function significantly increased from 1.34 (0.76) %/min/m2 at baseline to 1.56 (0.75) %/min/m2 6 weeks after RE (P = 0.024). The mean (SD) functional volume (liver volume minus tumor volume) of the left liver lobe significantly increased from baseline (407.3 [170.3] mL) to follow-up (499.1 [209.8] mL; P < 0.01), with an equivalent magnitude to the metabolic function increase. There were no reports of grade ≥3 adverse events.
Conclusion: This study indicates that unilobar RE produces a significant increase in the metabolic function, and equivalent volume increase, of the contralateral lobe. RE may be a useful option to induce hypertrophy of the future liver remnant before surgical resection of primary or secondary liver malignancies.
Copyright © 2021 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
B.G. has received research grants from Sirtex Medical as well as lecture honoraria and travel grants from Sirtex Medical, Amgen, Merck, Roche, Novartis and B. Braun Travacare, and receives honoraria for participation on advisory boards from Terumo, Sirtex Medical and Amgen. H.A. receives lecture fees from Norgine, Pfizer, Novartis, GE, Sirtex Medical as well as research grants from Pfizer. R.D. receives lecture honoraria from Sirtex Medical. M.P. receives research grants from Bayer and Sirtex Medical as well as lecture honoraria from Sirtex Medical. M.S. receives research grants from Bayer and Sirtex Medical as well as lecture honoraria from Siemens, Cook, Boston Scientific, Sirtex Medical, Falk Foundation, Bayer and receives honoraria for participation on advisory boards from Sirtex Medical, Bayer and Siemens. The remaining authors declare that they have nothing to disclose.
Figures
References
-
- Abulkhir A, Limongelli P, Healey AJ, et al. Preoperative portal vein embolization for major liver resection: a meta-analysis. Ann Surg. 2008;247:49–57. - PubMed
-
- Denys A, Prior J, Bize P, et al. Portal vein embolization: what do we know? Cardiovasc Intervent Radiol. 2012;35:999–1008. - PubMed
-
- Elias D, De Baere T, Roche A, et al. During liver regeneration following right portal embolization the growth rate of liver metastases is more rapid than that of the liver parenchyma. Br J Surg. 1999;86:784–788. - PubMed
-
- Hoekstra LT, van Lienden KP, Doets A, et al. Tumor progression after preoperative portal vein embolization. Ann Surg. 2012;256:812–817. - PubMed
LinkOut - more resources
Full Text Sources
