

Clinical magnetocardiography: the unshielded bet-past, present, and future
- PMID: 37636301
- PMCID: PMC10448194
- DOI: 10.3389/fcvm.2023.1232882
Clinical magnetocardiography: the unshielded bet-past, present, and future
Abstract
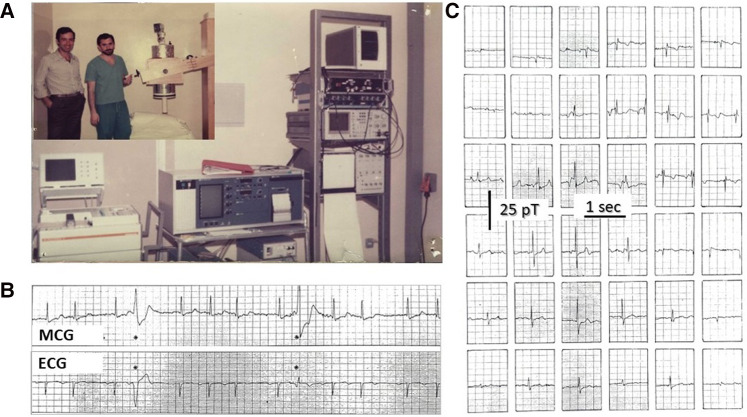
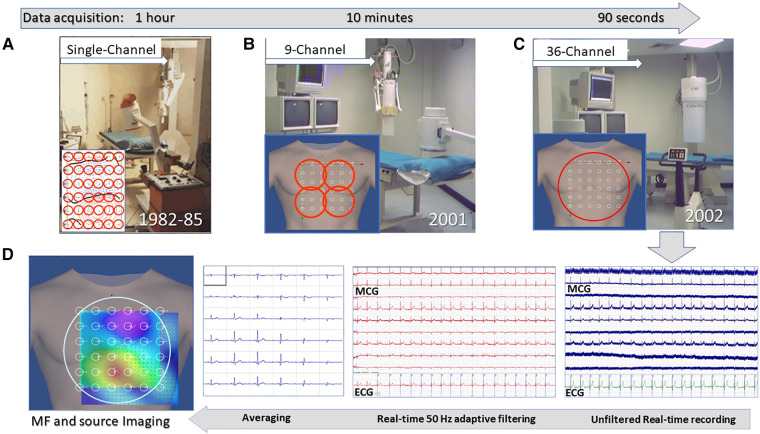
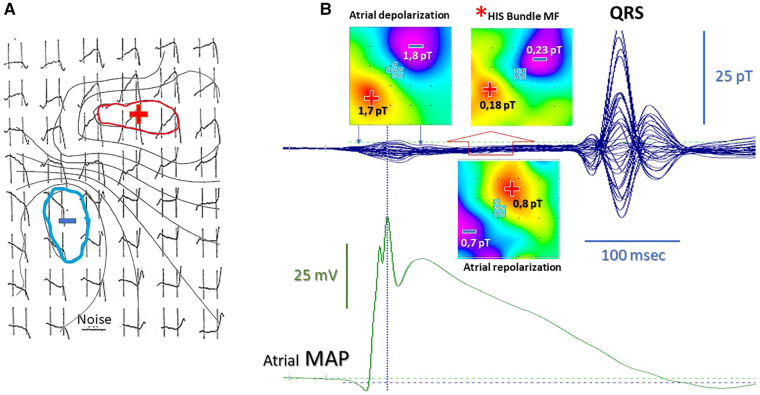
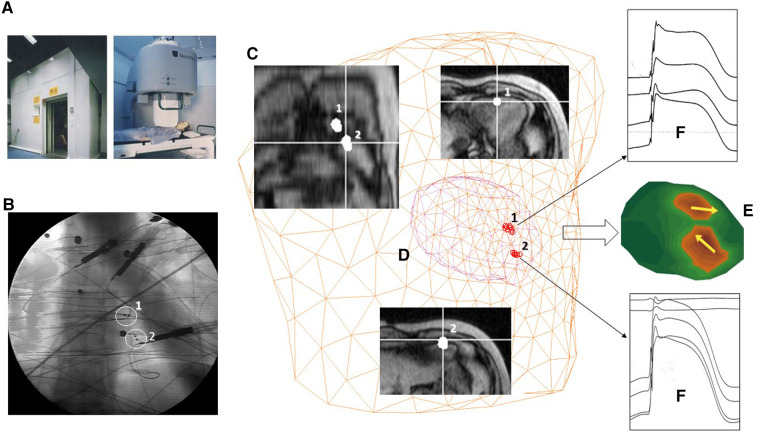
Magnetocardiography (MCG), which is nowadays 60 years old, has not yet been fully accepted as a clinical tool. Nevertheless, a large body of research and several clinical trials have demonstrated its reliability in providing additional diagnostic electrophysiological information if compared with conventional non-invasive electrocardiographic methods. Since the beginning, one major objective difficulty has been the need to clean the weak cardiac magnetic signals from the much higher environmental noise, especially that of urban and hospital environments. The obvious solution to record the magnetocardiogram in highly performant magnetically shielded rooms has provided the ideal setup for decades of research demonstrating the diagnostic potential of this technology. However, only a few clinical institutions have had the resources to install and run routinely such highly expensive and technically demanding systems. Therefore, increasing attempts have been made to develop cheaper alternatives to improve the magnetic signal-to-noise ratio allowing MCG in unshielded hospital environments. In this article, the most relevant milestones in the MCG's journey are reviewed, addressing the possible reasons beyond the currently long-lasting difficulty to reach a clinical breakthrough and leveraging the authors' personal experience since the early 1980s attempting to finally bring MCG to the patient's bedside for many years thus far. Their nearly four decades of foundational experimental and clinical research between shielded and unshielded solutions are summarized and referenced, following the original vision that MCG had to be intended as an unrivaled method for contactless assessment of the cardiac electrophysiology and as an advanced method for non-invasive electroanatomical imaging, through multimodal integration with other non-fluoroscopic imaging techniques. Whereas all the above accounts for the past, with the available innovative sensors and more affordable active shielding technologies, the present demonstrates that several novel systems have been developed and tested in multicenter clinical trials adopting both shielded and unshielded MCG built-in hospital environments. The future of MCG will mostly be dependent on the results from the ongoing progress in novel sensor technology, which is relatively soon foreseen to provide multiple alternatives for the construction of more compact, affordable, portable, and even wearable devices for unshielded MCG inside hospital environments and perhaps also for ambulatory patients.
Keywords: electroanatomical imaging; electrophysiology arrhythmias mapping and ablation; gradiometer array; inverse problem; magnetic sensors; magnetically shielded room (MSR); magnetocardiography (MCG); source localization accuracy.
© 2023 Brisinda, Fenici and Fenici.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Malmivuo J, Plonsey R. Bioelectromagnetism—principles and applications of bioelectric and biomagnetic fields (1995). BioLabor Biofizikai és Laboratóriumi Szolg. Kft. Available at: www.biolabor.hu. (last accessed 02 July 2023)
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous