

Case Report: Middle lobe syndrome: a rare presentation in eosinophilic granulomatosis with polyangiitis
- PMID: 37638004
- PMCID: PMC10448582
- DOI: 10.3389/fimmu.2023.1222431
Case Report: Middle lobe syndrome: a rare presentation in eosinophilic granulomatosis with polyangiitis
Abstract
Background: Antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) is a group of disorders characterized by necrotizing inflammation of small- and medium-sized blood vessels and the presence of circulating ANCA. Eosinophilic granulomatosis with polyangiitis (EGPA) is a systemic ANCA-associated vasculitis, characterized by peripheral eosinophilia, neuropathy, palpable purpuras or petechiae, renal and cardiac involvement, sinusitis, asthma, and transient pulmonary infiltrates. Middle lobe syndrome (MLS) is defined as recurrent or chronic atelectasis of the right middle lobe of the lung, and it is a potential complication of asthma.
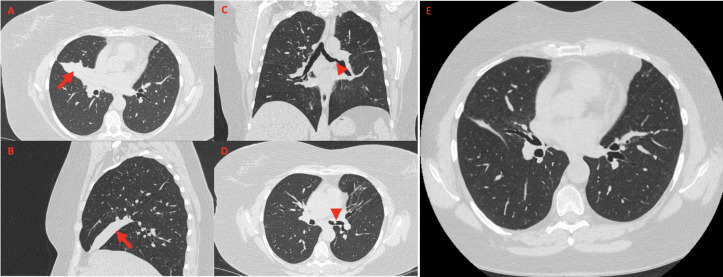
Case presentation: Herein, we describe a case of MLS in a 51-year-old woman, never-smoker, affected by EGPA, presenting exclusively with leukocytosis and elevated concentrations of acute-phase proteins, without any respiratory symptom, cough, or hemoptysis. Chest computed tomography (CT) imaging documented complete atelectasis of the middle lobe, together with complete obstruction of lobar bronchial branch origin. Fiberoptic bronchoscopy (FOB) revealed complete stenosis of the middle lobar bronchus origin, thus confirming the diagnosis of MLS, along with distal left main bronchus stenosis. Bronchoalveolar lavage (BAL) did not detect any infection. Bronchial biopsies included plasma cells, neutrophil infiltrates, only isolated eosinophils, and no granulomas, providing the hypothesis of vasculitic acute involvement less likely. First-line agents directed towards optimizing pulmonary function (mucolytics, bronchodilators, and antibiotic course) were therefore employed. However, the patient did not respond to conservative treatment; hence, endoscopic management of airway obstruction was performed, with chest CT documenting resolution of middle lobe atelectasis.
Conclusion: To the best of our knowledge, this is the first detailed description of MLS in EGPA completely resolved through FOB. Identification of MLS in EGPA appears essential as prognosis, longitudinal management, and treatment options may differ from other pulmonary involvement in AAV patients.
Keywords: Churg–Strauss; EGPA; asthma; eosinophilic granulomatosis with polyangiitis; middle lobe syndrome.
Copyright © 2023 Maranini, Guzzinati, Casoni, Ballotta, Lo Monaco and Govoni.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



References
-
- Grayson PC, Ponte C, Suppiah R, Robson JC, Craven A, Judge A, et al. . American College of rheumatology/european alliance of associations for rheumatology classification criteria for eosinophilic granulomatosis with polyangiitis. Ann Rheum Dis (2022. 2022) 81(3):309–14. doi: 10.1136/annrheumdis-2021-221794 - DOI - PubMed