

Haemodynamic effects of methoxyflurane versus fentanyl and placebo in hypovolaemia: a randomised, double-blind crossover study in healthy volunteers
- PMID: 37638077
- PMCID: PMC10457468
- DOI: 10.1016/j.bjao.2023.100204
Haemodynamic effects of methoxyflurane versus fentanyl and placebo in hypovolaemia: a randomised, double-blind crossover study in healthy volunteers
Abstract
Background: Methoxyflurane is approved for relief of moderate to severe pain in conscious adult trauma patients: it may be self-administrated and is well suited for use in austere environments. Trauma patients may sustain injuries causing occult haemorrhage compromising haemodynamic stability, and it is therefore important to elucidate whether methoxyflurane may adversely affect the haemodynamic response to hypovolaemia.
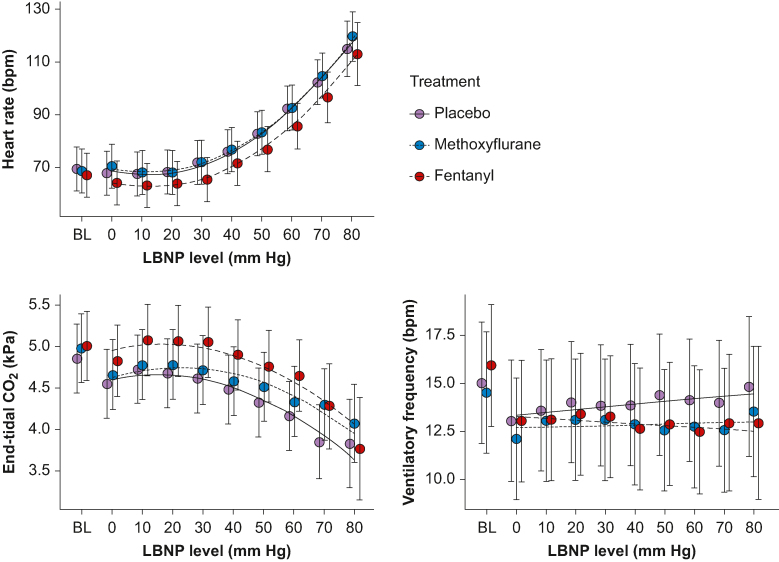
Methods: In this randomised, double-blinded, placebo-controlled, three-period crossover study, inhaled methoxyflurane 3 ml, i.v. fentanyl 25 μg, and placebo were administered to 15 healthy volunteers exposed to experimental hypovolaemia in the lower body negative pressure model. The primary endpoint was the effect of treatment on changes in cardiac output, while secondary endpoints were changes in stroke volume and mean arterial pressure and time to haemodynamic decompensation during lower body negative pressure.
Results: There were no statistically significant effects of treatment on the changes in cardiac output, stroke volume, or mean arterial pressure during lower body negative pressure. The time to decompensation was longer for methoxyflurane compared with fentanyl (hazard ratio 1.9; 95% confidence interval 0.4-3.4; P=0.010), whereas there was no significant difference to placebo (hazard ratio -1.3; 95% confidence interval -2.8 to 0.23; P=0.117).
Conclusions: The present study does not indicate that methoxyflurane has significant adverse haemodynamic effects in conscious adults experiencing hypovolaemia.
Clinical trial registration: ClinicalTrials.gov (NCT04641949) and EudraCT (2019-004144-29) https://www.clinicaltrialsregister.eu/ctr-search/trial/2019-004144-29/NO.
Keywords: analgesia; cardiac output; healthy volunteers; hypovolaemia; methoxyflurane.
© 2023 The Author(s).
Figures





References
-
- Sauaia A., Moore F.A., Moore E.E., et al. Epidemiology of trauma deaths: a reassessment. J Trauma Acute Care Surg. 1995;38:185–193. - PubMed
-
- Wedmore I.S., Butler F.K. Battlefield analgesia in tactical combat casualty care. Wilderness Environ Med. 2017;28:S109–S116. - PubMed
-
- Thomas S.H., Shewakramani S. Prehospital trauma analgesia. J Emerg Med. 2008;35:47–57. - PubMed
-
- Albrecht E., Taffe P., Yersin B., Schoettker P., Decosterd I., Hugli O. Undertreatment of acute pain (oligoanalgesia) and medical practice variation in prehospital analgesia of adult trauma patients: a 10 yr retrospective study. Br J Anaesth. 2013;110:96–106. - PubMed
-
- Stephen C. Clinical applications of methoxyflurane. Acta Anaesthesiol Scand. 1966;10:215–222. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
