

Over diagnosis of bradykinin angioedema in patients treated with angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers
- PMID: 37638360
- PMCID: PMC10458346
- DOI: 10.1016/j.waojou.2023.100809
Over diagnosis of bradykinin angioedema in patients treated with angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers
Abstract
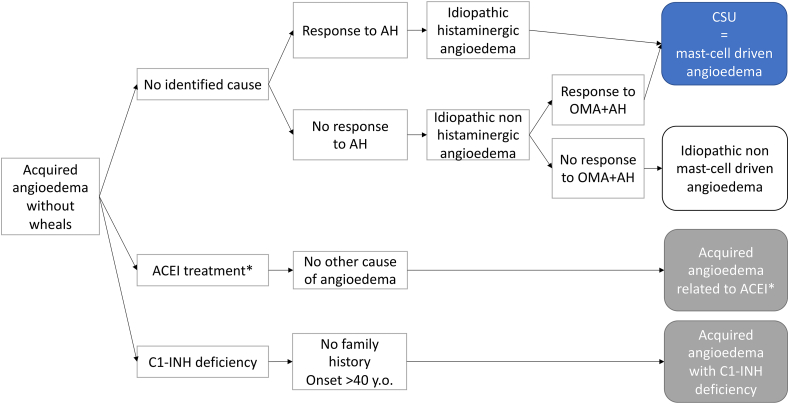
Background: Bradykinin angioedemas are a potentially serious side effect of angiotensin-converting enzyme inhibitors (ACEI) and more controversially of angiotensin II receptor blockers (ARB). Their challenging diagnosis is based on the absence of any recurrence after more than 6 months of drug discontinuation; otherwise mast-cell driven angioedemas as a differential diagnosis must be considered.
Objective: The aim of this study was to determine the prevalence of recurrent angioedema in patients referred for ACEI/ARB-induced bradykinin angioedema, after more than 6 months of drug discontinuation.
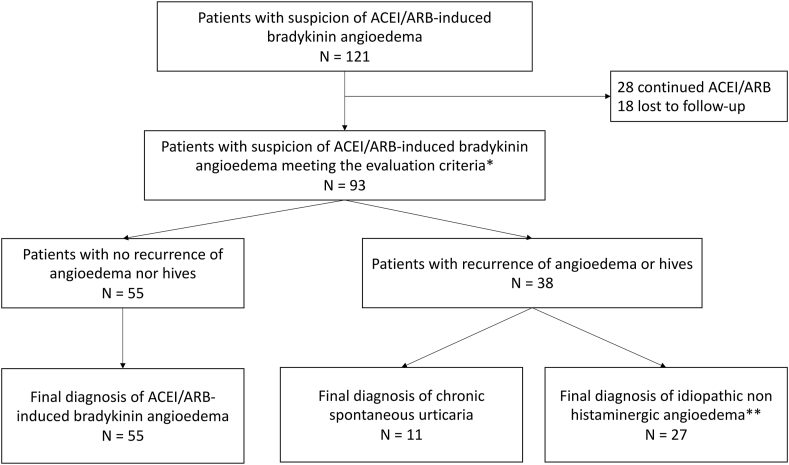
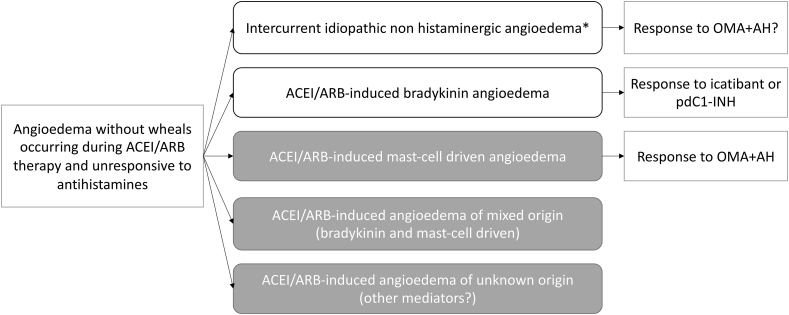
Methods: We included ACEI/ARB-treated patients referred for angioedema(s) without hives and unresponsive to antihistamines, after they discontinued ACEI/ARB for at least 6 months. Any C1-inhibitor deficiency was excluded. The primary endpoint was the prevalence of patients with recurrent angioedema after more than 6 months of drug discontinuation and/or developing hives during follow-up. The secondary endpoint was the identification of epidemiological factors associated with any final diagnosis.
Results: Thirty-eight of 93 patients (41%) with a suspicion of ACEI/ARB-induced bradykinin angioedema still had recurrent angioedema (n = 27) or developed hives (n = 2) or both (n = 9) after 6 months of drug discontinuation. Good response to icatibant and facial but not oral localization were predictive for the final diagnosis of ACEI/ARB-induced bradykinin angioedema and mast-cell driven angioedema, respectively.
Conclusion: In patients referred for acquired angioedema without wheals occurring during ACEI/ARB therapy, 59% finally had a diagnosis of ACEI/ARB-induced bradykinin angioedema whereas 41% were rather diagnosed with mast-cell driven angioedema. The overdiagnosis of ACEI/ARB-induced bradykinin angioedema may deteriorate the management of severe cardiovascular conditions.
Keywords: Angioedema; Angiotensin converting enzyme inhibitors; Bradykinin; Mast-cell; Urticaria.
© 2023 Published by Elsevier Inc. on behalf of World Allergy Organization.
Conflict of interest statement
None.
Figures
Similar articles
-
ACE inhibitor-mediated angioedema.Int Immunopharmacol. 2020 Jan;78:106081. doi: 10.1016/j.intimp.2019.106081. Epub 2019 Dec 10. Int Immunopharmacol. 2020. PMID: 31835086 Review.
-
Molecular Genetic Screening in Patients With ACE Inhibitor/Angiotensin Receptor Blocker-Induced Angioedema to Explore the Role of Hereditary Angioedema Genes.Front Genet. 2022 Jul 18;13:914376. doi: 10.3389/fgene.2022.914376. eCollection 2022. Front Genet. 2022. PMID: 35923707 Free PMC article.
-
Managing Chronic Urticaria and Recurrent Angioedema Differently with Advancing Age.J Allergy Clin Immunol Pract. 2021 Jun;9(6):2186-2194. doi: 10.1016/j.jaip.2021.03.034. Epub 2021 Apr 2. J Allergy Clin Immunol Pract. 2021. PMID: 33819638
-
Angioedema Triggered by Medication Blocking the Renin/Angiotensin System: Retrospective Study Using the French National Pharmacovigilance Database.J Clin Immunol. 2016 Jan;36(1):95-102. doi: 10.1007/s10875-015-0228-3. Epub 2015 Dec 28. J Clin Immunol. 2016. PMID: 26707788
-
Angiotensin-converting enzyme inhibitor-induced angioedema: A review of the literature.J Clin Hypertens (Greenwich). 2017 Dec;19(12):1377-1382. doi: 10.1111/jch.13097. Epub 2017 Oct 10. J Clin Hypertens (Greenwich). 2017. PMID: 28994183 Free PMC article. Review.
Cited by
-
Five-Membered Nitrogen Heterocycles Angiotensin-Converting Enzyme (ACE) Inhibitors Induced Angioedema: An Underdiagnosed Condition.Pharmaceuticals (Basel). 2024 Mar 10;17(3):360. doi: 10.3390/ph17030360. Pharmaceuticals (Basel). 2024. PMID: 38543146 Free PMC article. Review.
-
Angiotensin-converting enzyme inhibitor-induced angioedema: Proposal for a diagnostic score.World Allergy Organ J. 2025 Mar 12;18(3):101037. doi: 10.1016/j.waojou.2025.101037. eCollection 2025 Mar. World Allergy Organ J. 2025. PMID: 40151541 Free PMC article.
-
Amlodipine-Associated Angioedema: An Integrated Pharmacovigilance Assessment Using Disproportionality and Interaction Analysis and Case Reviews.J Clin Med. 2025 Feb 8;14(4):1097. doi: 10.3390/jcm14041097. J Clin Med. 2025. PMID: 40004629 Free PMC article.
References
-
- Hoover T., Lippmann M., Grouzmann E., Marceau F., Herscu P. Angiotensin converting enzyme inhibitor induced angio-oedema: a review of the pathophysiology and risk factors. Clin Exp Allergy. 2010;40(1):50–61. - PubMed
-
- Dicpinigaitis P.V. Angiotensin-converting enzyme inhibitor-induced cough: ACCP evidence-based clinical practice guidelines. Chest. 2006 Jan 1;129(1, Supplement):169S–173S. - PubMed
-
- Caldeira D., David C., Sampaio C. Tolerability of angiotensin-receptor blockers in patients with intolerance to angiotensin-converting enzyme inhibitors. Am J Cardiovasc Drugs. 2012 Aug 1;12(4):263–277. - PubMed
LinkOut - more resources
Full Text Sources
