

Expanding HIV clinical monitoring: the role of CD4, CD8, and CD4/CD8 ratio in predicting non-AIDS events
- PMID: 37639938
- PMCID: PMC10474064
- DOI: 10.1016/j.ebiom.2023.104773
Expanding HIV clinical monitoring: the role of CD4, CD8, and CD4/CD8 ratio in predicting non-AIDS events
Abstract
Background: While a low CD4/CD8 ratio during HIV treatment correlates with immunosenescence, its value in identifying patients at an increased risk for clinical events remains unclear.
Methods: We analyzed data from the CoRIS cohort to determine whether CD4 count, CD8 count, and CD4/CD8 ratio at year two of antiretroviral therapy (ART) could predict the risk of serious non-AIDS events (SNAEs) during the next five years. These included major adverse cardiovascular events, non-AIDS-defining malignancies, and non-accidental deaths. We used pooled logistic regression with inverse probability weighting to estimate the survival curves and cumulative risk of clinical events.
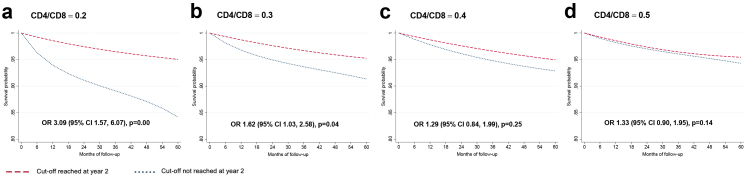
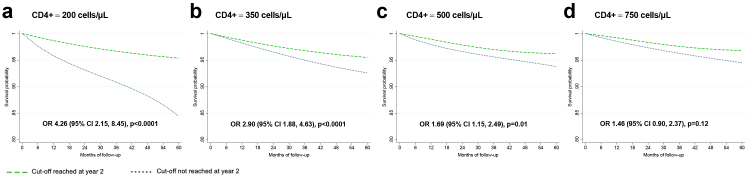
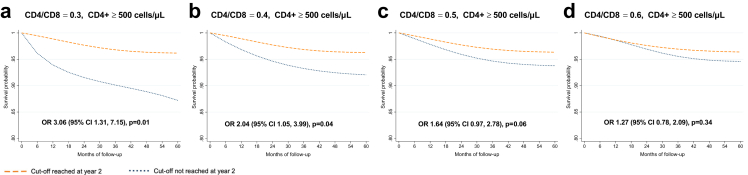
Findings: The study included 4625 participants, 83% male, of whom 200 (4.3%) experienced an SNAE during the follow-up period. A CD4/CD8 ratio <0.3 predicted an increased risk of SNAEs during the next five years (OR 1.63, 95% CI 1.03-2.58). The effect was stronger at a CD4/CD8 ratio cut-off of <0.2 (OR 3.09, 95% CI 1.57-6.07). Additionally, low CD4 count at cut-offs of <500 cells/μL predicted an increased risk of clinical events. Among participants with a CD4 count ≥500 cells/μL, a CD8 count ≥1500 cells/μL or a CD4/CD8 ratio <0.4 predicted increased SNAE risk.
Interpretation: Our results support the use of the CD4/CD8 ratio and CD8 count as predictors of clinical progression. Patients with CD4/CD8 ratio <0.3 or CD8 count ≥1500/μL, regardless of their CD4 count, may benefit from closer monitoring and targeted preventive interventions.
Funding: This work was supported by CIBER (CB 2021), Instituto de Salud Carlos III, Ministerio de Ciencia e Innovación and Unión Europea-NextGenerationEU; by the Spanish AIDS Research Network (RIS) RD16/0025/0001 project as part of the Plan Nacional R + D + I, and cofinanced by Instituto de Salud Carlos III (ISCIII)- Subdirección General de Evaluación y el Fondo Europeo de Desarrollo Regional (FEDER), ISCIII projects PI18/00154, PI21/00141, and ERDF, "A way to make Europe", ICI20/00058.
Keywords: CD4/CD8 ratio; Cardiovascular event; HIV; Neoplasia; Non-AIDS events.
Copyright © 2023 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests J.M.-S. reports personal fees from ViiV Healthcare, Janssen Cilag, Gilead Sciences, and MSD, non-financial support from ViiV Healthcare, Jannsen Cilag, and Gilead Sciences, and research grants from Gilead Sciences, outside the submitted work. S. S.-V. reports personal fees from Gilead Sciences, MSD, Mikrobiomik, and Aptatargets, non-financial support from ViiV Healthcare and Gilead Sciences, and research grants from MSD and Gilead Sciences, outside the submitted work. S.M. reports grants, personal fees and non-financial support from ViiV Healthcare, personal fees, and non-financial support from Janssen, grants, personal fees and non-financial support from MSD, grants, personal fees, and non-financial support from Gilead, outside the submitted work. F.G. reports personal fees and non-financial support from ViiV Healthcare and Janssen Cilag.
Figures
References
-
- Lewden C., Bouteloup V., De Wit S., et al. All-cause mortality in treated HIV-infected adults with CD4 ≥500/mm3 compared with the general population: evidence from a large European observational cohort collaboration. Int J Epidemiol. 2012;41:433–445. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
