

ECAP-controlled closed-loop versus open-loop SCS for the treatment of chronic pain: 36-month results of the EVOKE blinded randomized clinical trial
- PMID: 37640452
- PMCID: PMC11103285
- DOI: 10.1136/rapm-2023-104751
ECAP-controlled closed-loop versus open-loop SCS for the treatment of chronic pain: 36-month results of the EVOKE blinded randomized clinical trial
Abstract
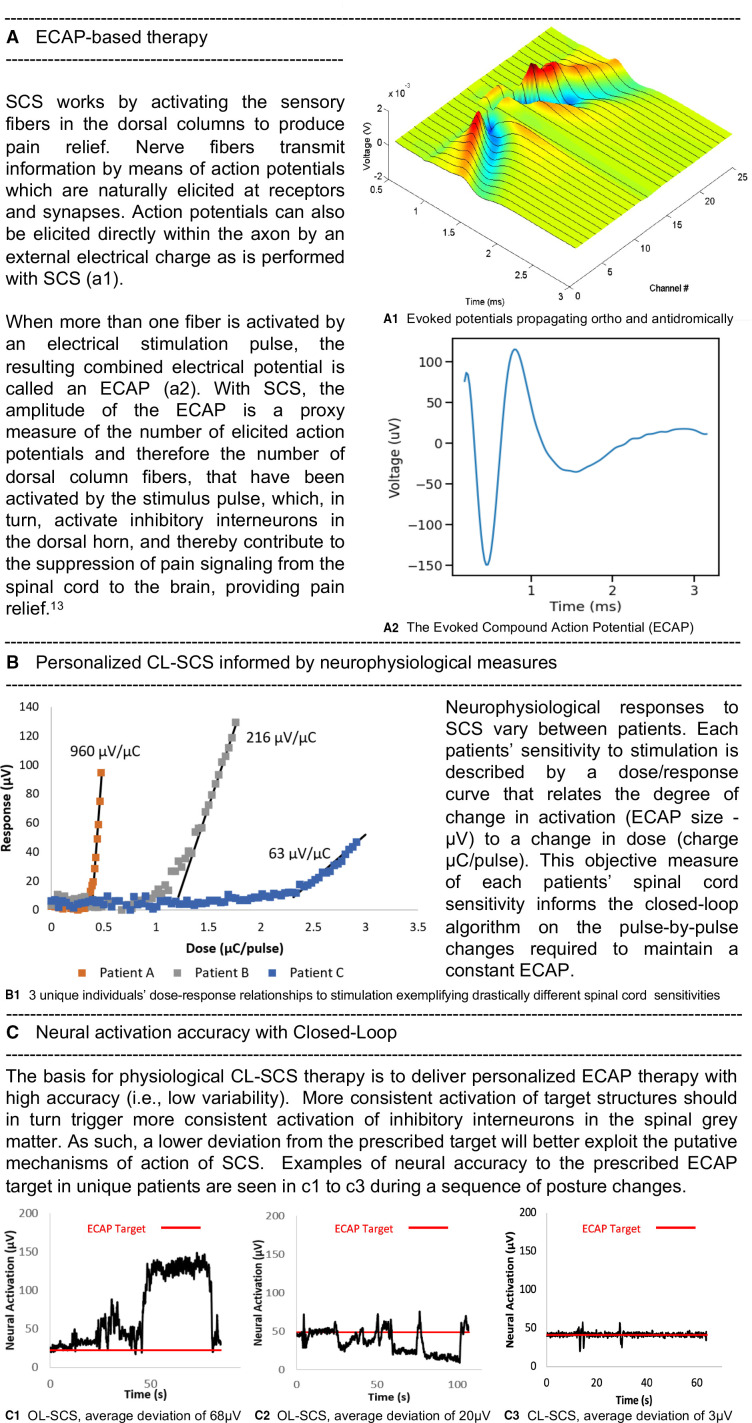
Introduction: The evidence for spinal cord stimulation (SCS) has been criticized for the absence of blinded, parallel randomized controlled trials (RCTs) and limited evaluations of the long-term effects of SCS in RCTs. The aim of this study was to determine whether evoked compound action potential (ECAP)-controlled, closed-loop SCS (CL-SCS) is associated with better outcomes when compared with fixed-output, open-loop SCS (OL-SCS) 36 months following implant.
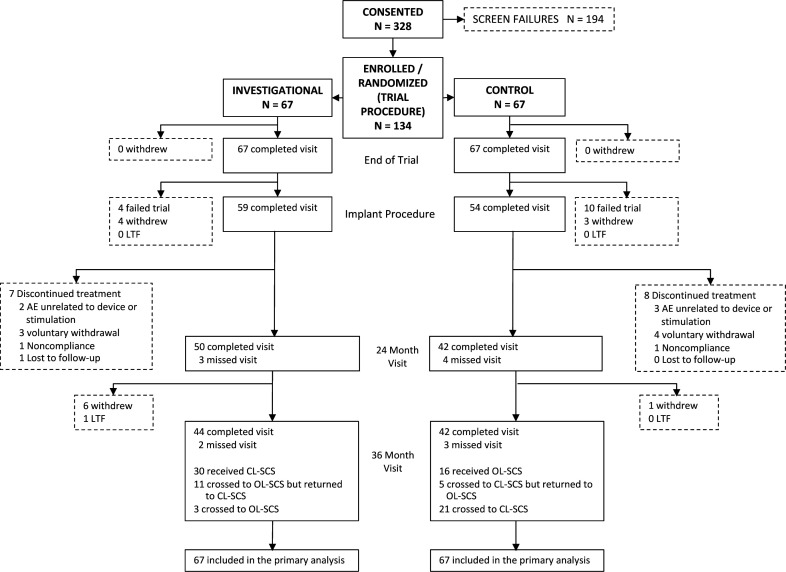
Methods: The EVOKE study was a multicenter, participant-blinded, investigator-blinded, and outcome assessor-blinded, randomized, controlled, parallel-arm clinical trial that compared ECAP-controlled CL-SCS with fixed-output OL-SCS. Participants with chronic, intractable back and leg pain refractory to conservative therapy were enrolled between January 2017 and February 2018, with follow-up through 36 months. The primary outcome was a reduction of at least 50% in overall back and leg pain. Holistic treatment response, a composite outcome including pain intensity, physical and emotional functioning, sleep, and health-related quality of life, and objective neural activation was also assessed.
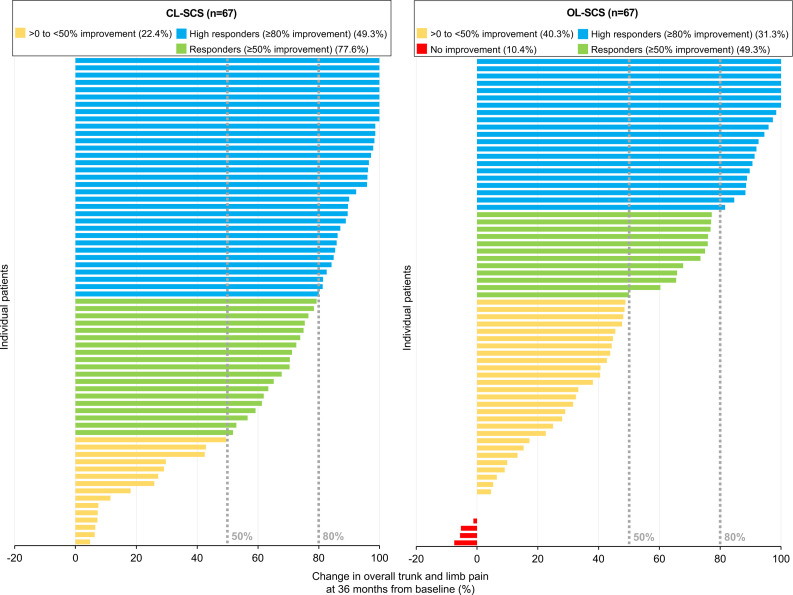
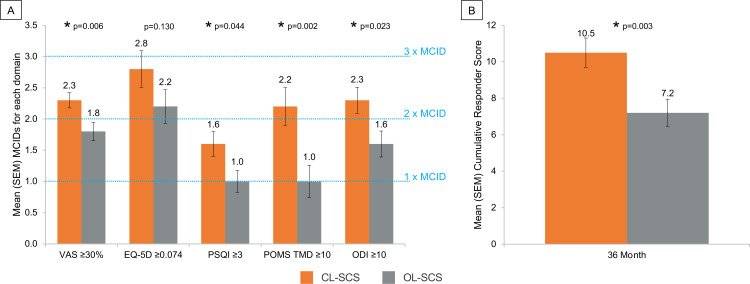
Results: At 36 months, more CL-SCS than OL-SCS participants reported ≥50% reduction (CL-SCS=77.6%, OL-SCS=49.3%; difference: 28.4%, 95% CI 12.8% to 43.9%, p<0.001) and ≥80% reduction (CL-SCS=49.3%, OL-SCS=31.3%; difference: 17.9, 95% CI 1.6% to 34.2%, p=0.032) in overall back and leg pain intensity. Clinically meaningful improvements from baseline were observed at 36 months in both CL-SCS and OL-SCS groups in all other patient-reported outcomes with greater levels of improvement with CL-SCS. A greater proportion of patients with CL-SCS were holistic treatment responders at 36-month follow-up (44.8% vs 28.4%), with a greater cumulative responder score for CL-SCS patients. Greater neural activation and accuracy were observed with CL-SCS. There were no differences between CL-SCS and OL-SCS groups in adverse events. No explants due to loss of efficacy were observed in the CL-SCS group.
Conclusion: This long-term evaluation with objective measurement of SCS therapy demonstrated that ECAP-controlled CL-SCS resulted in sustained, durable pain relief and superior holistic treatment response through 36 months. Greater neural activation and increased accuracy of therapy delivery were observed with ECAP-controlled CL-SCS than OL-SCS.
Trial registration number: NCT02924129.
Keywords: CHRONIC PAIN; Neuromodulation; Spinal Cord Stimulation.
© American Society of Regional Anesthesia & Pain Medicine 2024. Re-use permitted under CC BY-NC. No commercial re-use. Published by BMJ.
Conflict of interest statement
Competing interests: NM reports personal fees from Saluda Medical for acting as independent medical monitor for the EVOKE study during the conduct of the study; he reports receiving grants from Neuros and Mesoblast, as well as consulting as a medical monitor for Nevro, Vivex, Mainstay, and Vertos outside the submitted work. RL is an uncompensated consultant for Nalu, Saluda Medical, and Mainstay Medical and has stock options from Nalu and Saluda Medical obtained before 2019, not exercisable through the duration of his term as International Neuromodulation Society President and editor-in-chief of the journal Neuromodulation: Technology at the Neural Interface. TD reports personal fees from Saluda Medical during the conduct of the study; consultancy for Axonics, Abbott, Nalu, Vertos, SpineThera, Mainstay, Cornerloc, Ethos, SPR Therapeutics, Medtronic, Boston Scientific, PainTeq, Tissue Tech, Spinal Simplicity, and Avanos outside the submitted work. He is a minor equity holder for Saluda Medical, Nalu, SpineThera, Stimgenics, Vertiflex, Vertos, and Bioness and an advisory board member for Abbott, Vertos, Nalu, SPR Therapeutics, and Tissue Tech. LK reports receiving grants from Nevro, Neuros, Avanos, Medtronic, Neuralace, and Xalud Therapeutics and financial support from Nevro, Avanos, and Saluda Medical outside the submitted work. SL reports receiving grants and personal fees from Saluda Medical during the conduct of the study; he reports grants from Avanos, Boston Scientific, Nalu Medical, SPR Therapeutics, Averitas Pharma, Biotronik, SGX Therapeutics, and PainTeq, as well as consultancy for Abbott, Avanos, Boston Scientific, Nevro, SPR Therapeutics, Averitas Pharma, Biotronik, Nalu Medical, and PainTeq, outside the submitted work, as well as holding stock options for Nalu Medical. KA reports consultancy for Medtronic, Nevro, Boston Scientific, Nalu, Presidio, Biotronik, Mesoblast, Vivex Laboratories outside the submitted work. JP reports research and consulting fees from Saluda Medical during the conduct of the study; consultancy for Abbott, Medtronic, Saluda Medical, Flowonix, SpineThera, Vertos, Vertiflex, SPR Therapeutics, Tersera, Aurora, Spark, Ethos, Biotronik, Mainstay, WISE, Boston Scientific, and Thermaquil outside the submitted work; has received grant and research support from: Abbott, Flowonix, Aurora, Painteq, Ethos, Muse, Boston Scientific, SPR Therapeutics, Mainstay, Vertos, AIS, and Thermaquil outside the submitted work; and is a shareholder of Vertos, SPR Therapeutics, Painteq, Aurora, Spark, Celeri Health, Neural Integrative Solutions, Pacific Research Institute, Thermaquil, and Anesthetic Gas Reclamation. CH reports grants from Saluda Medical during the conduct of the study; consultancy fees from Genecentrix outside the submitted work. SC reports grants from Cleveland Clinic during the conduct of the study; and grants from Vertos, Mainstay, and Vivex outside the submitted work. SMF reports consulting fees from Abbott, Medtronic, Saluda, VertiFlex, Vertos, Surgentec, CornerLoc, Mainstay and Relievant outside the submitted work, has received grant for research funding from Mainstay, Relievant, Medtronic, Abbott, VertiFlex, Saluda, Nalu, CornerLoc, Aurora, Biotronik, and Stimgenics outside the submitted work, and has an equity position in SynerFuse, Aurora Spine, Thermaquil. SPR Therapeutics, Saluda, CornerLoc, PainTEQ, Stimgenics, Anesthetic Gas Reclamation, Neural Integrative Solutions, SpineThera, and Celeri Health. CG reports clinical trial funding from Saluda Medical during the conduct of the study; reports personal fees and other from SPR, and personal fees from Nevro, Nalu, Biotronik, and Boston Scientific outside the submitted work. PSS has received consultancy fees from Medtronic, Saluda Medical, Nalu, and Biotronic outside the submitted work, and has stock options from Saluda Medical and Nalu. JS reports personal fees from Nevro during the conduct of the study and personal fees from Saluda Medical and Boston Scientific outside the submitted work. TM reports research fees from Saluda Medical during the conduct of the study and personal fees from Nevro outside the submitted work. JC reports personal fees from Saluda Medical during the conduct of the study; personal fees from Abbott, Boston Scientific, Nevro, Medtronic, Mainstay, SPR Therapeutics, CornerLoc, PillNurse, Biotronik, and Vivex outside the submitted work; and stock from Mainstay, CornerLoc, and PillNurse. EP has received research support from Mainstay, Medtronic, Neuros Medical, Nevro Corp, ReNeuron, SPR, and Saluda Medical outside the submitted work, as well as personal fees from Abbott Neuromodulation, Biotronik, Medtronic Neuromodulation, Nalu, Neuros Medical, Nevro, Presidio Medical, Saluda Medical, and Vertos outside the submitted work. She holds stock options from SynerFuse and neuro42. JMH reports consulting fees from Abbott, Boston Scientific, Nevro, and Saluda Medical outside the submitted work. RR reports grants from SPR, Nalu and Nevro outside the submitted work,l fees from Presidio, and grants and personal fees from Boston Scientific and Saluda Medical outside the submitted work. JWK is an advisory board member for Boston Scientific, Medtronic, Abbott, and Saluda Medical. GB reports consulting fees from Medtronic, Boston Scientific, and Saluda Medical outside the submitted work, and has a consulting agreement and is on the advisory board for Nevro Corp, Nalu Medical Inc, Abbott, and Boston Scientific. RST reports consulting fees from Medtronic, Nevro and Saluda Medical outside the submitted work. LP reports personal fees from Saluda Medical; is a member of the data monitoring board of Saluda Medical during the conduct of the study; and reports personal consulting fees from Medtronic and Nalu outside the submitted work. Members of the EVOKE study group report being employees of Saluda Medical. No other disclosures were reported.
Figures
References
-
- National Institute for Health and Care Excellence (NICE) . Spinal cord stimulation for chronic pain of neuropathic or ischaemic origin. Technology appraisal guidance [TA159]. 2008. Available: https://www.nice.org.uk/guidance/ta159 [Accessed 31 Oct 2022].
-
- Shealy CN, Mortimer JT, Reswick JB. Electrical inhibition of pain by stimulation of the dorsal columns: preliminary clinical report. Anesth Analg 1967;46:489–91. - PubMed
-
- Katz N, Dworkin RH, North R, et al. . Research design considerations for randomized controlled trials of spinal cord stimulation for pain: initiative on methods, measurement, and pain assessment in clinical trials/Institute of neuromodulation/International neuromodulation society recommendations. Pain 2021;162:1935–56. 10.1097/j.pain.0000000000002204 - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical