

Anesthetic management of scapular Y-osteotomy using a combination of suprascapular nerve block and erector spinae plane block for Sprengel deformity associated with Klippel-Feil syndrome: a case report
- PMID: 37640974
- PMCID: PMC10462535
- DOI: 10.1186/s40981-023-00647-3
Anesthetic management of scapular Y-osteotomy using a combination of suprascapular nerve block and erector spinae plane block for Sprengel deformity associated with Klippel-Feil syndrome: a case report
Abstract
Background: Klippel-Feil syndrome (KFS) occurs in 1/40,000 individuals and is characterized by cervical fusion. Thirty percent of patients with KFS present with Sprengel deformity, leading to orthopedic problems and limited shoulder abduction. No reports exist regarding anesthetic procedures for pediatric scapular osteotomies.
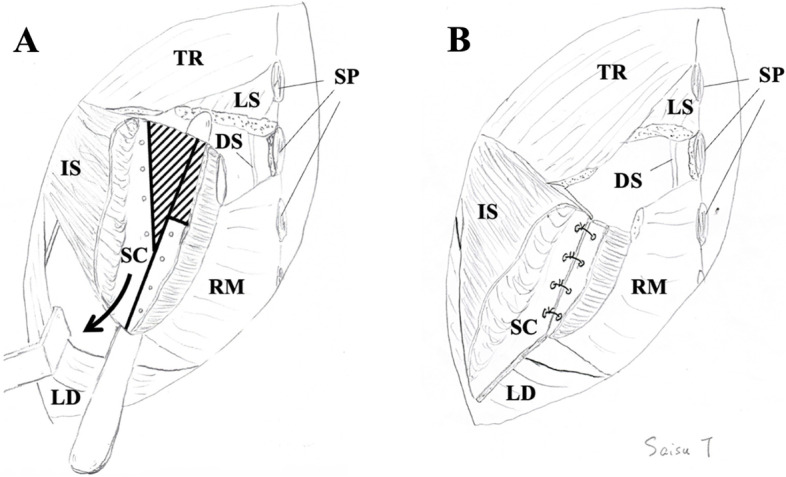
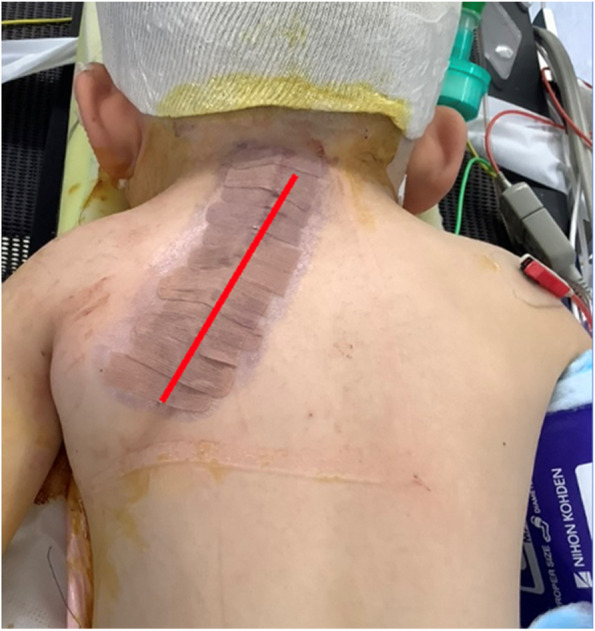
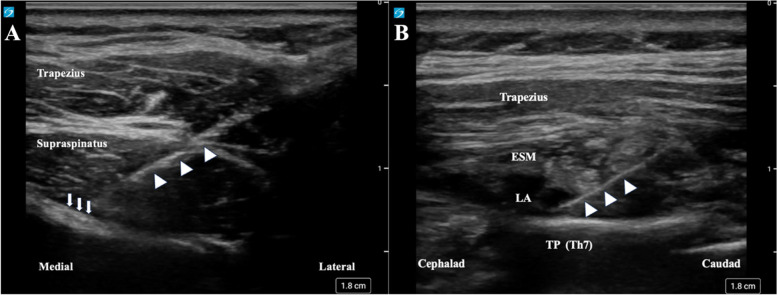
Case presentation: We report a case of a 4-year-and-7-month-old boy (95.6 cm, 14.7 kg) who underwent left scapular osteotomy. At the age of 8 months, he also underwent a right lower lobectomy due to a congenital pulmonary airway malformation. We decided to use a combination of suprascapular nerve block (SSNB), erector spinae plane block (ESPB), and general anesthesia. He received regular acetaminophen administration and fentanyl 5-10 μg/hour intravenously until 20 h postoperatively and remained on ≤ 2/10 in the Wong-Baker Face Scale (0: no hurt; 10: hurts worst).
Conclusion: The combination of SSNB and ESPB could be an option for perioperative analgesia for scapular osteotomies.
Keywords: Erector spinae plane block; Pediatric anesthesia; Peripheral nerve block; Suprascapular nerve block.
© 2023. The Japanese Society of Anesthesiologists.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
LinkOut - more resources
Full Text Sources