

Hysteroscopic management of uterine diverticulum after myomectomy: a case report
- PMID: 37641054
- PMCID: PMC10464432
- DOI: 10.1186/s12905-023-02606-7
Hysteroscopic management of uterine diverticulum after myomectomy: a case report
Abstract
Background: A uterine diverticulum is defined as the presence of a niche within the inner contour of the uterine myometrial wall. Although secondary uterine diverticula can occur after hysterotomy such as cesarean section, reports of diverticula after myomectomy are extremely rare.
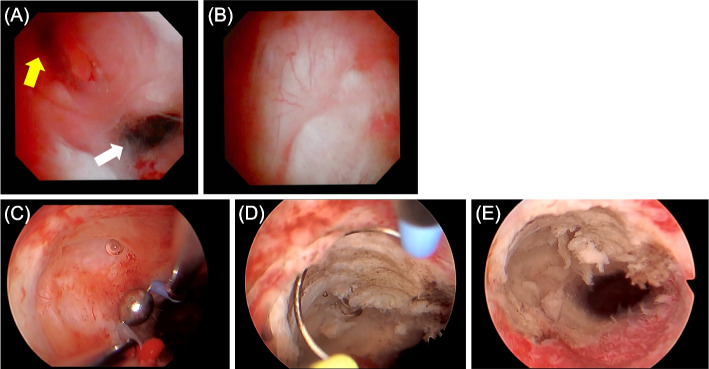
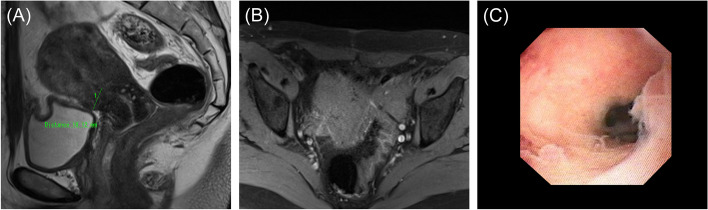
Case presentation: A 45-year-old nulliparous woman undergoing infertility treatment was referred to our hospital because of abnormal postmenstrual bleeding after myomectomy. Transvaginal sonography and magnetic resonance imaging revealed a diverticulum in the isthmus. Fat-saturated T1 image showed a blood reservoir in the diverticulum. Hysteroscopic surgery was performed to remove the lowed edge of the defect and coagulate the hypervascularized area. Two months after surgery, the abnormal postmenstrual bleeding and chronic endometritis improved.
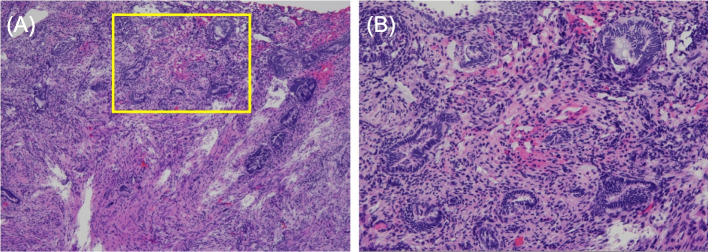
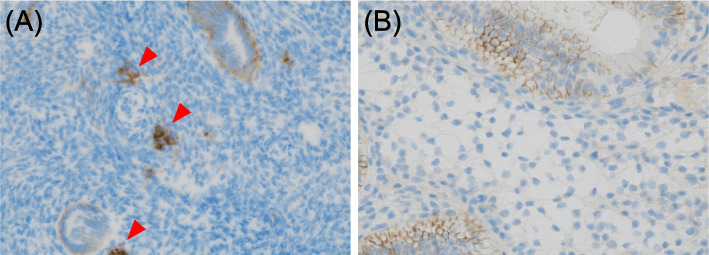
Discussion and conclusions: This report highlights the similarities of the patient's diverticulum to cesarean scar defects in terms of symptoms and pathophysiology. First, this patient developed a diverticulum with hypervascularity after myomectomy and persistent abnormal bleeding. Second, after hysteroscopic surgery, the symptoms of irregular bleeding disappeared. Third, endometrial glands were identified within the resected scar tissue. Fourth, preoperatively identified CD138-positive cells in endometrial tissue spontaneously disappeared after hysteroscopic resection. To the best of our knowledge, this is the first report of symptomatic improvement following hysteroscopic surgery in a patient with an iatrogenic uterine diverticulum with persistent irregular bleeding after myomectomy.
Keywords: Cesarean scar defect; Hysteroscopic surgery; Myomectomy; Uterine diverticulum.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
Successful surgical treatment of postmyomectomy uterine diverticulum: a case report.BMC Womens Health. 2023 Aug 3;23(1):406. doi: 10.1186/s12905-023-02539-1. BMC Womens Health. 2023. PMID: 37537601 Free PMC article.
-
Iatrogenic Uterine Diverticulum in Pregnancy After Robotic-assisted Myomectomy.J Minim Invasive Gynecol. 2015 Jul-Aug;22(5):902-5. doi: 10.1016/j.jmig.2015.03.016. Epub 2015 Mar 28. J Minim Invasive Gynecol. 2015. PMID: 25827328
-
Treatment of uterine scar cystoid diverticulum by hysteroscopy combined with laparoscopy.Fertil Steril. 2023 Oct;120(4):922-924. doi: 10.1016/j.fertnstert.2023.07.013. Epub 2023 Jul 25. Fertil Steril. 2023. PMID: 37499779
-
Placental Invasion into the Small Bowel Intestine Through a Myomectomy Scar: A Case Report With Literature Review.Int J Gynecol Pathol. 2022 Mar 1;41(2):151-156. doi: 10.1097/PGP.0000000000000778. Int J Gynecol Pathol. 2022. PMID: 33782340 Review.
-
Uterine scar rupture - Prediction, prevention, diagnosis, and management.Best Pract Res Clin Obstet Gynaecol. 2019 Aug;59:115-131. doi: 10.1016/j.bpobgyn.2019.01.009. Epub 2019 Feb 10. Best Pract Res Clin Obstet Gynaecol. 2019. PMID: 30837118 Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
