

An AI-powered patient triage platform for future viral outbreaks using COVID-19 as a disease model
- PMID: 37641126
- PMCID: PMC10463861
- DOI: 10.1186/s40246-023-00521-4
An AI-powered patient triage platform for future viral outbreaks using COVID-19 as a disease model
Abstract
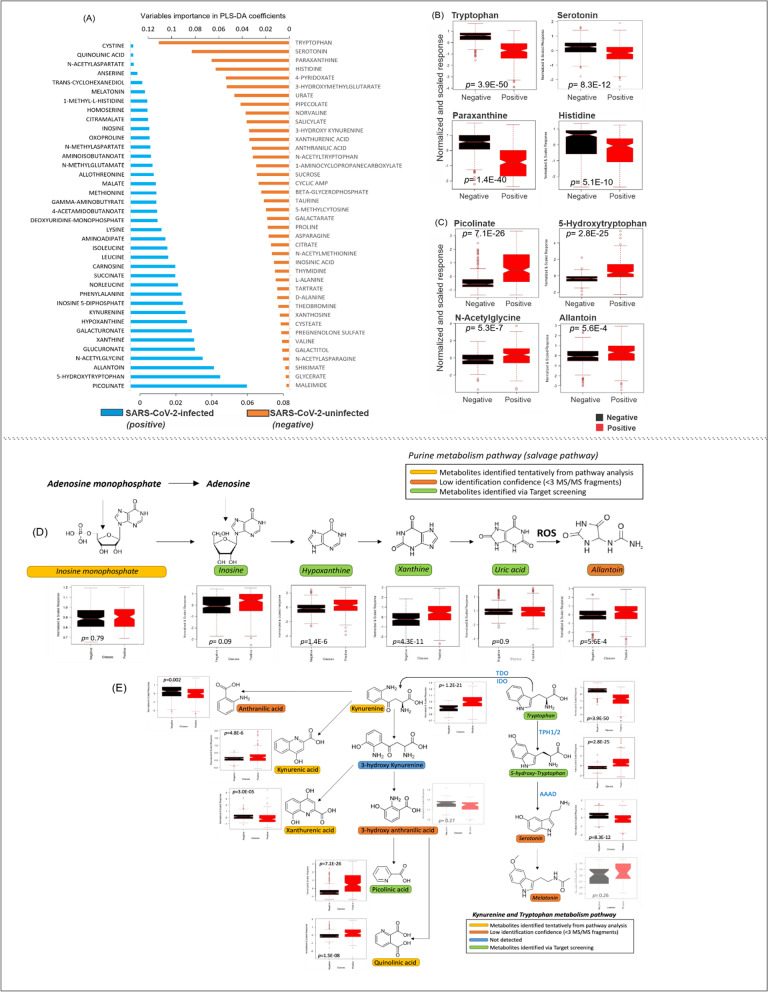
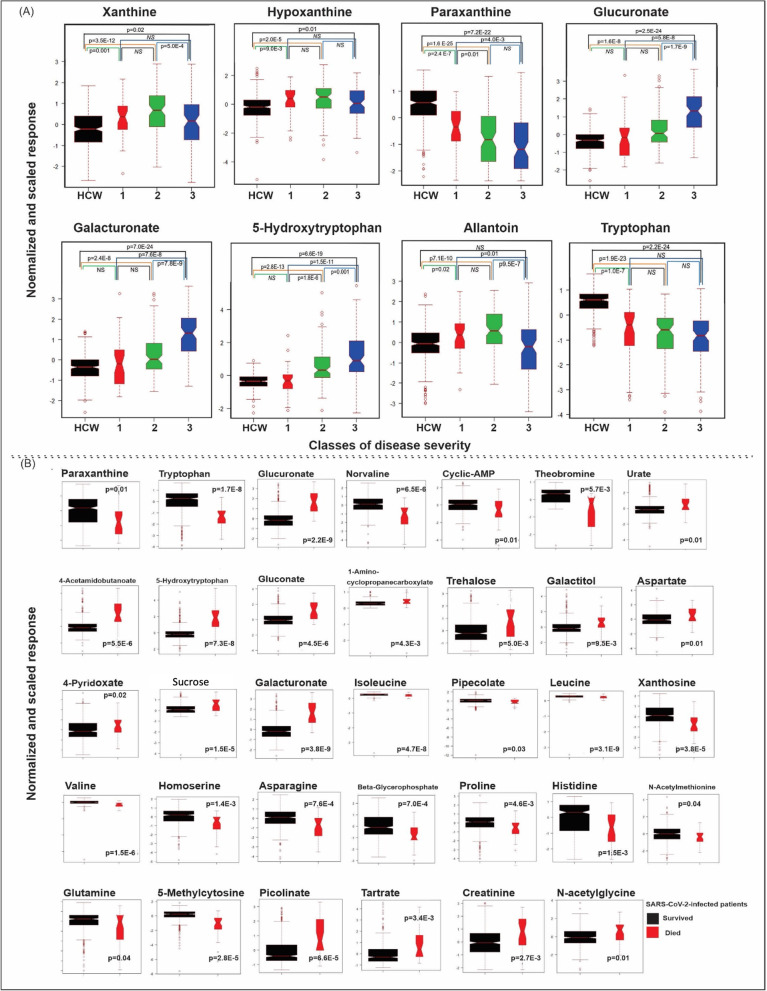
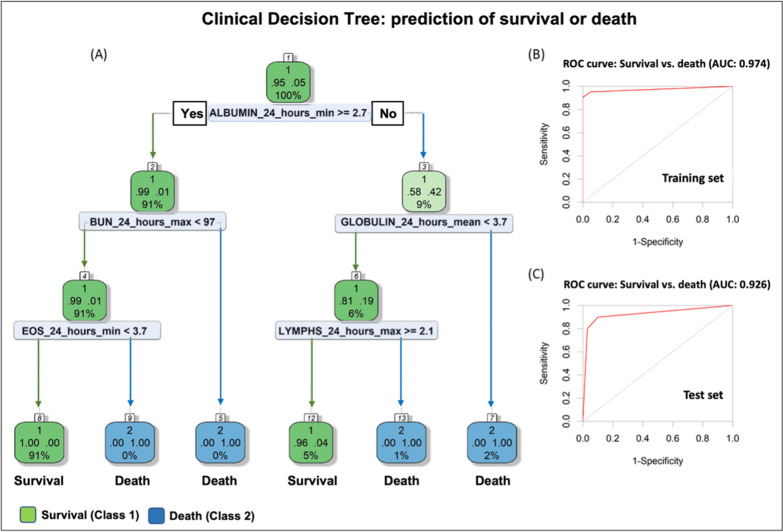
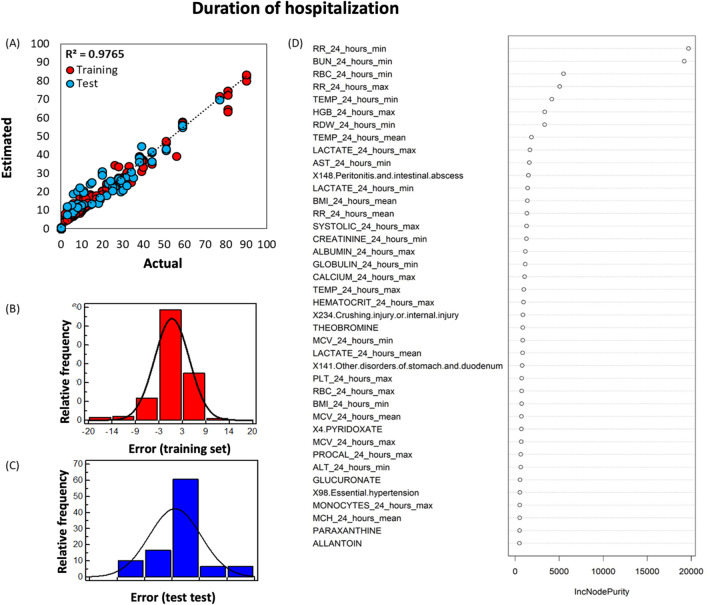
Over the last century, outbreaks and pandemics have occurred with disturbing regularity, necessitating advance preparation and large-scale, coordinated response. Here, we developed a machine learning predictive model of disease severity and length of hospitalization for COVID-19, which can be utilized as a platform for future unknown viral outbreaks. We combined untargeted metabolomics on plasma data obtained from COVID-19 patients (n = 111) during hospitalization and healthy controls (n = 342), clinical and comorbidity data (n = 508) to build this patient triage platform, which consists of three parts: (i) the clinical decision tree, which amongst other biomarkers showed that patients with increased eosinophils have worse disease prognosis and can serve as a new potential biomarker with high accuracy (AUC = 0.974), (ii) the estimation of patient hospitalization length with ± 5 days error (R2 = 0.9765) and (iii) the prediction of the disease severity and the need of patient transfer to the intensive care unit. We report a significant decrease in serotonin levels in patients who needed positive airway pressure oxygen and/or were intubated. Furthermore, 5-hydroxy tryptophan, allantoin, and glucuronic acid metabolites were increased in COVID-19 patients and collectively they can serve as biomarkers to predict disease progression. The ability to quickly identify which patients will develop life-threatening illness would allow the efficient allocation of medical resources and implementation of the most effective medical interventions. We would advocate that the same approach could be utilized in future viral outbreaks to help hospitals triage patients more effectively and improve patient outcomes while optimizing healthcare resources.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
VV, KV NST are members of the editorial board of Human Genomics.
Figures
Similar articles
-
Development and evaluation of a machine learning-based in-hospital COVID-19 disease outcome predictor (CODOP): A multicontinental retrospective study.Elife. 2022 May 17;11:e75985. doi: 10.7554/eLife.75985. Elife. 2022. PMID: 35579324 Free PMC article.
-
The future of Cochrane Neonatal.Early Hum Dev. 2020 Nov;150:105191. doi: 10.1016/j.earlhumdev.2020.105191. Epub 2020 Sep 12. Early Hum Dev. 2020. PMID: 33036834
-
Development of a clinical decision support system for severity risk prediction and triage of COVID-19 patients at hospital admission: an international multicentre study.Eur Respir J. 2020 Aug 20;56(2):2001104. doi: 10.1183/13993003.01104-2020. Print 2020 Aug. Eur Respir J. 2020. PMID: 32616597 Free PMC article.
-
A Machine Learning Approach to Predicting Need for Hospitalization for Pediatric Asthma Exacerbation at the Time of Emergency Department Triage.Acad Emerg Med. 2018 Dec;25(12):1463-1470. doi: 10.1111/acem.13655. Epub 2018 Nov 29. Acad Emerg Med. 2018. PMID: 30382605
-
Allocation of intensive care resources during an infectious disease outbreak: a rapid review to inform practice.BMC Med. 2020 Dec 18;18(1):404. doi: 10.1186/s12916-020-01871-9. BMC Med. 2020. PMID: 33334347 Free PMC article. Review.
Cited by
-
Isotopic Ratio Outlier Analysis (IROA) for Quantitative Analysis.Methods Mol Biol. 2025;2925:69-89. doi: 10.1007/978-1-0716-4534-5_4. Methods Mol Biol. 2025. PMID: 40498181
-
Transformative Potential of AI in Healthcare: Definitions, Applications, and Navigating the Ethical Landscape and Public Perspectives.Healthcare (Basel). 2024 Jan 5;12(2):125. doi: 10.3390/healthcare12020125. Healthcare (Basel). 2024. PMID: 38255014 Free PMC article. Review.
-
Severity Patterns in COVID-19 Hospitalised Patients in Spain: I-MOVE-COVID-19 Study.Viruses. 2024 Oct 30;16(11):1705. doi: 10.3390/v16111705. Viruses. 2024. PMID: 39599820 Free PMC article.
-
CYP2E1 in 1,4-dioxane metabolism and liver toxicity: insights from CYP2E1 knockout mice study.Arch Toxicol. 2024 Oct;98(10):3241-3257. doi: 10.1007/s00204-024-03811-5. Epub 2024 Aug 27. Arch Toxicol. 2024. PMID: 39192018
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
