

Subclinical cardiac dysfunction may impact on fluid and vasopressor administration during early resuscitation of septic shock
- PMID: 37641139
- PMCID: PMC10463881
- DOI: 10.1186/s44158-023-00117-3
Subclinical cardiac dysfunction may impact on fluid and vasopressor administration during early resuscitation of septic shock
Abstract
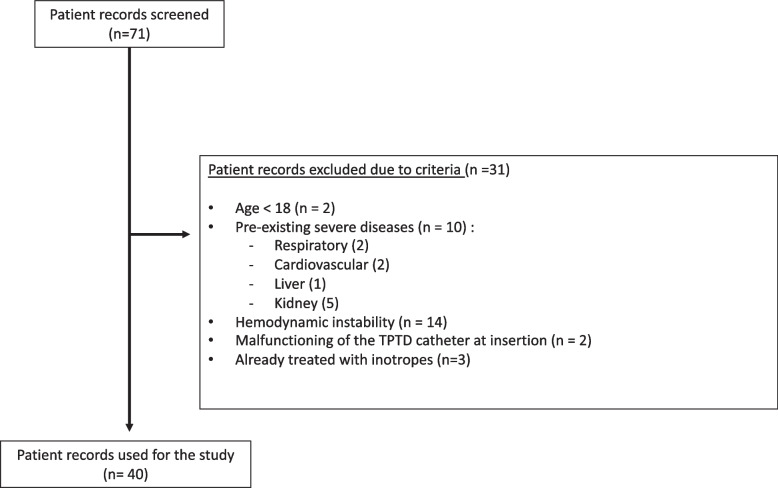
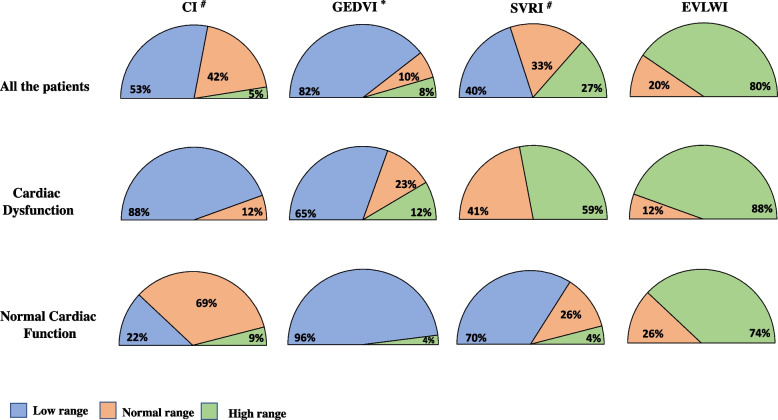
Background: According to the Surviving Sepsis Campaign (SSC) fluids and vasopressors are the mainstays of early resuscitation of septic shock while inotropes are indicated in case of tissue hypoperfusion refractory to fluids and vasopressors, suggesting severe cardiac dysfunction. However, septic cardiac disfunction encompasses a large spectrum of severities and may remain "subclinical" during early resuscitation. We hypothesized that "subclinical" cardiac dysfunction may nevertheless influence fluid and vasopressor administration during early resuscitation. We retrospectively reviewed prospectically collected data on fluids and vasoconstrictors administered outside the ICU in patients with septic shock resuscitated according to the SSC guidelines that had reached hemodynamic stability without the use of inotropes. All the patients were submitted to transpulmonary thermodilution (TPTD) hemodynamic monitoring at ICU entry. Subclinical cardiac dysfunction was defined as a TPTD-derived cardiac function index (CFI) ≤ 4.5 min-1.
Results: At ICU admission, subclinical cardiac dysfunction was present in 17/40 patients (42%; CFI 3.6 ± 0.7 min-1 vs 6.6 ± 1.9 min-1; p < 0.01). Compared with patients with normal CFI, these patients had been resuscitate with more fluids (crystalloids 57 ± 10 vs 47 ± 9 ml/kg PBW; p < 0.01) and vasopressors (norepinephrine 0.65 ± 0.25 vs 0.43 ± 0.29 mcg/kg/min; p < 0.05). At ICU admission these patients had lower cardiac index (2.2 ± 0.6 vs 3.6 ± 0.9 L/min/m2, p < 0.01) and higher systemic vascular resistances (2721 ± 860 vs 1532 ± 480 dyn*s*cm-5/m2, p < 0.01).
Conclusions: In patients with septic shock resuscitated according to the SSC, we found that subclinical cardiac dysfunction may influence the approach to fluids and vasopressor administration during early resuscitation. Our data support the implementation of early, bedside assessment of cardiac function during early resuscitation of septic shock.
Keywords: Hemodynamic resuscitation; Sepsis-related cardiac dysfunction; Septic shock; Surviving Sepsis Campaign; Trans-pulmonary thermodilution.
© 2023. Italian Society of Anesthesia, Analgesia, Resuscitation and Intensive Care.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous