

Endometriosis in the era of precision medicine and impact on sexual and reproductive health across the lifespan and in diverse populations
- PMID: 37641572
- PMCID: PMC10503213
- DOI: 10.1096/fj.202300907
Endometriosis in the era of precision medicine and impact on sexual and reproductive health across the lifespan and in diverse populations
Abstract
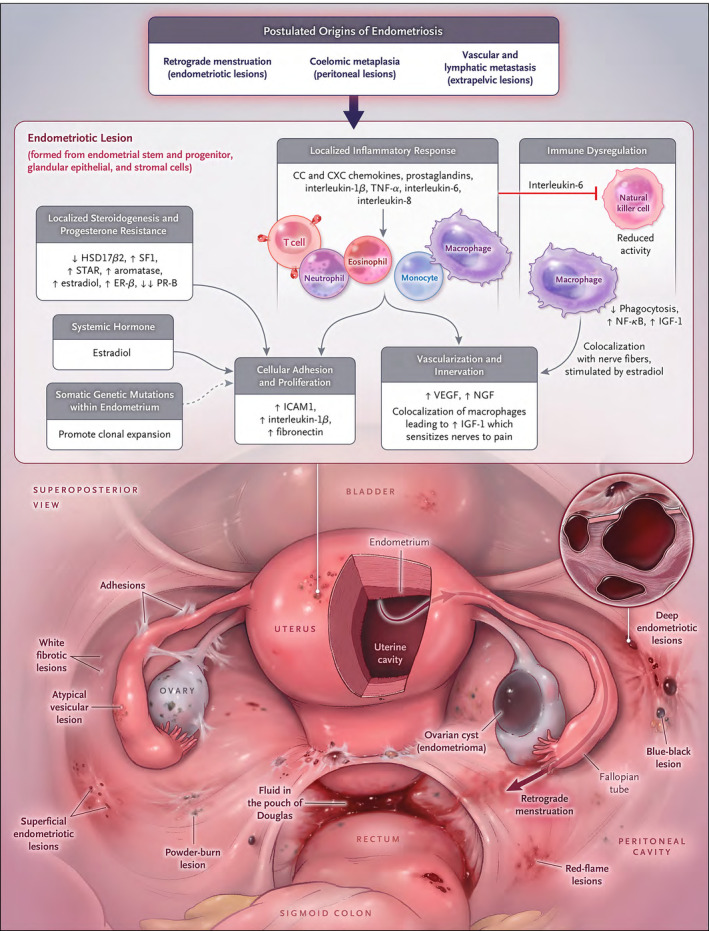
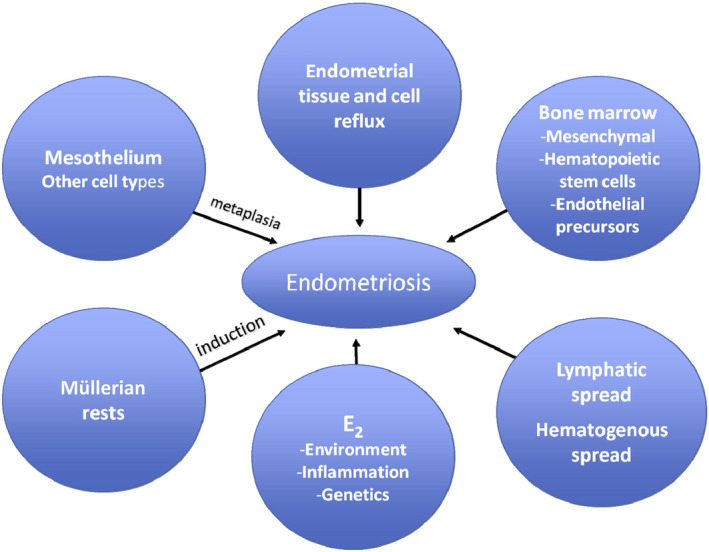
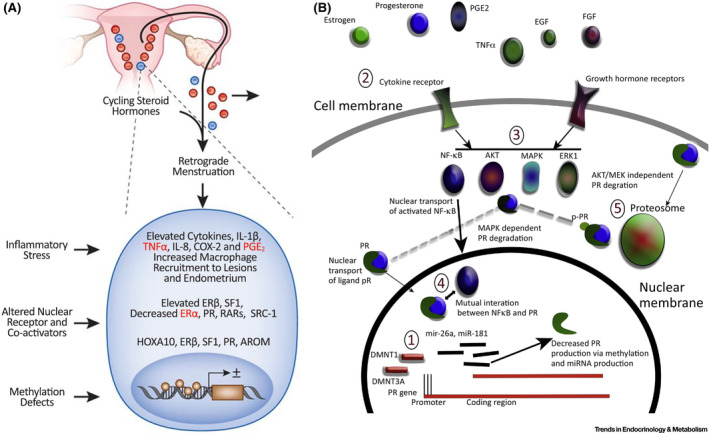
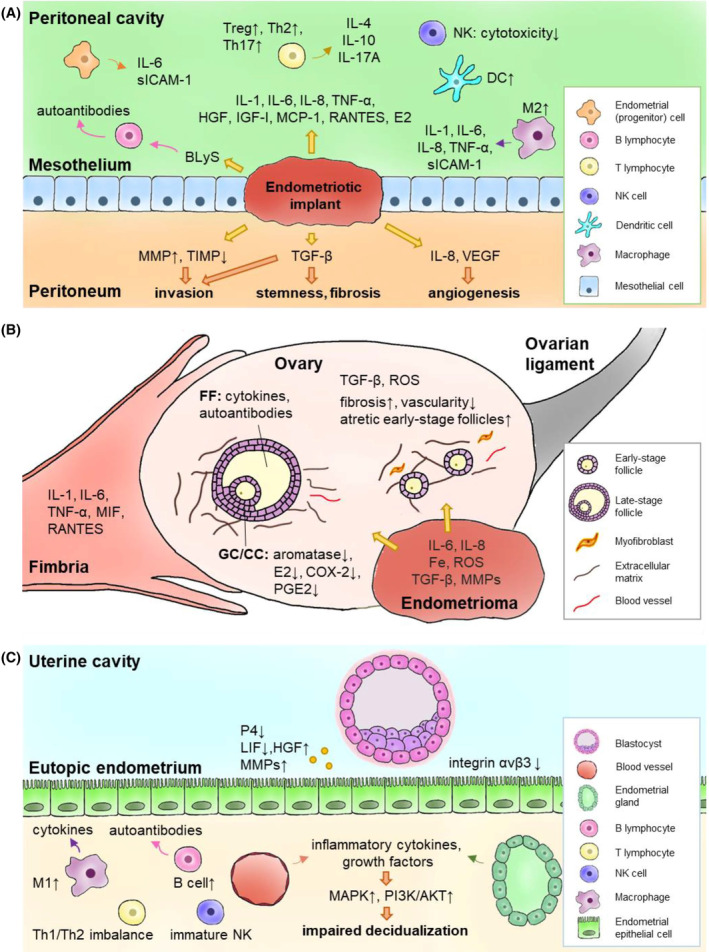
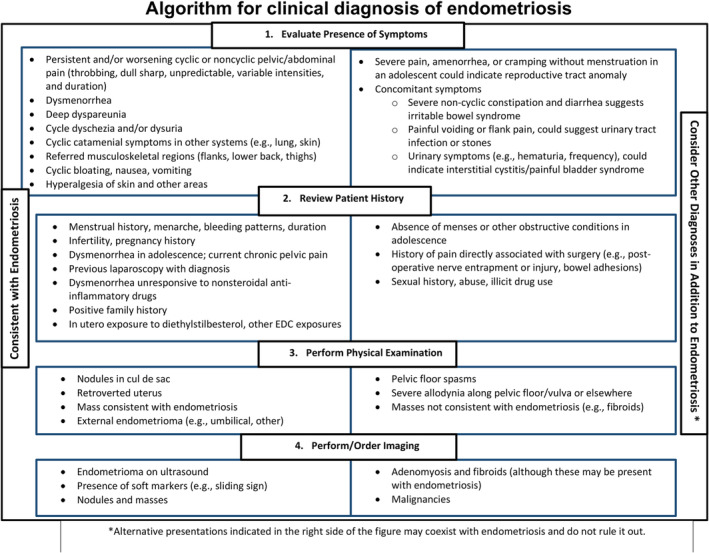
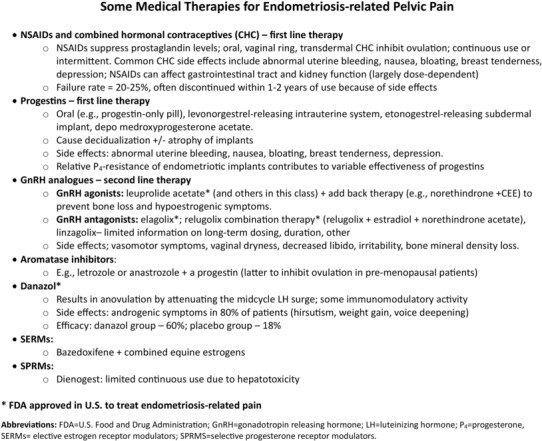
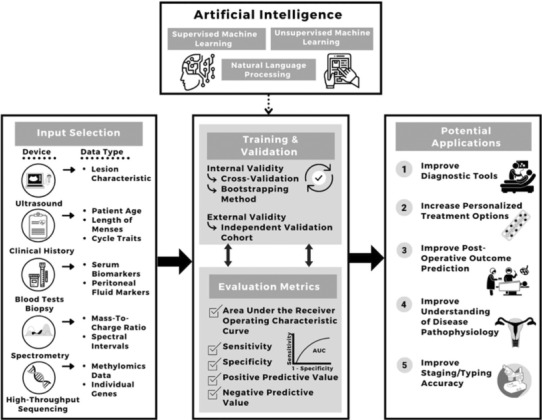
Endometriosis is a common estrogen-dependent disorder wherein uterine lining tissue (endometrium) is found mainly in the pelvis where it causes inflammation, chronic pelvic pain, pain with intercourse and menses, and infertility. Recent evidence also supports a systemic inflammatory component that underlies associated co-morbidities, e.g., migraines and cardiovascular and autoimmune diseases. Genetics and environment contribute significantly to disease risk, and with the explosion of omics technologies, underlying mechanisms of symptoms are increasingly being elucidated, although novel and effective therapeutics for pain and infertility have lagged behind these advances. Moreover, there are stark disparities in diagnosis, access to care, and treatment among persons of color and transgender/nonbinary identity, socioeconomically disadvantaged populations, and adolescents, and a disturbing low awareness among health care providers, policymakers, and the lay public about endometriosis, which, if left undiagnosed and under-treated can lead to significant fibrosis, infertility, depression, and markedly diminished quality of life. This review summarizes endometriosis epidemiology, compelling evidence for its pathogenesis, mechanisms underlying its pathophysiology in the age of precision medicine, recent biomarker discovery, novel therapeutic approaches, and issues around reproductive justice for marginalized populations with this disorder spanning the past 100 years. As we enter the next revolution in health care and biomedical research, with rich molecular and clinical datasets, single-cell omics, and population-level data, endometriosis is well positioned to benefit from data-driven research leveraging computational and artificial intelligence approaches integrating data and predicting disease risk, diagnosis, response to medical and surgical therapies, and prognosis for recurrence.
Keywords: access; biomarkers; diagnosis; diversity; endometriosis; equity; health disparities; precision medicine; therapies.
© 2023 The Authors. The FASEB Journal published by Wiley Periodicals LLC on behalf of Federation of American Societies for Experimental Biology.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
