

A preoperative predictive tool to assess the need for staging laparoscopy in oesophagogastric cancer patients
- PMID: 37642164
- PMCID: PMC10981985
- DOI: 10.1308/rcsann.2022.0140
A preoperative predictive tool to assess the need for staging laparoscopy in oesophagogastric cancer patients
Abstract
Introduction: Staging laparoscopy (SL) has become commonplace in the preoperative staging pathway for oesophagogastric (OG) cancer. SL is often performed before curative treatment to examine for macroscopic peritoneal metastases (PM) or positive peritoneal cytology (PPC). The aim of this study was to develop an objective risk scoring system to predict both PM and PPC at SL.
Methods: A prospectively collected and maintained database of all OG cancer patients treated between 2006 and 2020 was reviewed. Univariate and multivariate analyses were performed to identify risk factors for both PM and PPC at SL. A risk score was produced for both PM and PPC, and then validated internally.
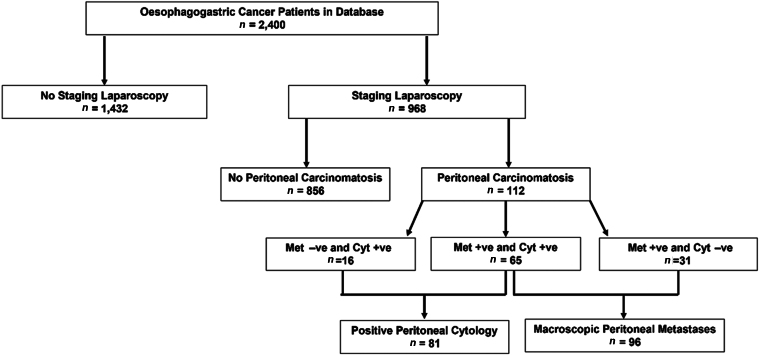
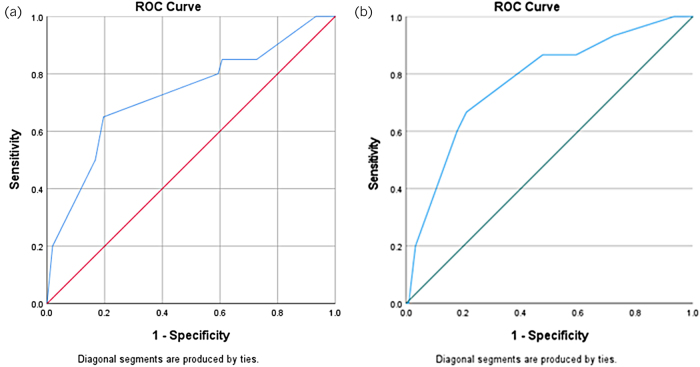
Results: Among 968 patients who underwent SL, 96 (9.9%) had PM and 81 (8.4%) had PPC at SL. Tumour site (p < 0.001), computed tomography (CT) T stage (p < 0.001) and N stage (p = 0.029) were significantly associated with PM at SL (p < 0.001). Tumour site (p < 0.001), biopsy histology (p = 0.041), CT T stage (p < 0.001) and N stage (p < 0.001) were significantly associated with PPC. The risk scoring model for PM included cancer site and CT T stage. This was successfully tested on the validation set (area under the receiver operating characteristic [AUROC] = 0.730). The risk scoring model for PPC included cancer site, CT T and N stage. This was successfully tested on the validation set (AUROC = 0.773).
Conclusions: The current risk scores are valid tools with which to predict the risk PM and PPC in patients undergoing SL for OG cancer and may help to avoid subjecting patients to unnecessary SL.
Keywords: Gastric cancer; Oesophageal cancer; Staging laparoscopy.
Figures
Similar articles
-
Multidetector Computed Tomography Versus Staging Laparoscopy for the Detection of Peritoneal Metastases in Esophagogastric Junctional and Gastric Cancer.Surg Laparosc Endosc Percutan Tech. 2017 Oct;27(5):369-374. doi: 10.1097/SLE.0000000000000451. Surg Laparosc Endosc Percutan Tech. 2017. PMID: 28787380
-
The incremental benefit of two quadrant lavage for peritoneal cytology at staging laparoscopy for oesophagogastric adenocarcinoma.Surg Endosc. 2013 Nov;27(11):4049-53. doi: 10.1007/s00464-013-3058-5. Epub 2013 Jul 9. Surg Endosc. 2013. PMID: 23836122
-
The neutrophil/lymphocyte ratio as a predictor of peritoneal metastasis during staging laparoscopy for advanced gastric cancer: a retrospective cohort analysis.World J Surg Oncol. 2019 Jun 25;17(1):108. doi: 10.1186/s12957-019-1651-3. World J Surg Oncol. 2019. PMID: 31238937 Free PMC article.
-
The role of laparoscopy and laparoscopic ultrasound in the preoperative staging of pancreatico-biliary cancers--A meta-analysis.Eur J Surg Oncol. 2010 Oct;36(10):941-8. doi: 10.1016/j.ejso.2010.05.015. Epub 2010 Jun 12. Eur J Surg Oncol. 2010. PMID: 20547445 Review.
-
The effects of staging laparoscopy on trocar site and peritoneal recurrence of pancreatic cancer.Surg Endosc. 2004 Feb;18(2):310-3. doi: 10.1007/s00464-003-8909-z. Epub 2003 Dec 29. Surg Endosc. 2004. PMID: 14691701 Review.
References
-
- Nath J, Moorthy K, Taniere Pet al. . Peritoneal lavage cytology in patients with oesophagogastric adenocarcinoma. Br J Surg 2008; 95: 721–726. - PubMed
-
- Allen CJ, Newhook TE, Vreeland TJet al. . Yield of peritoneal cytology in staging patients with gastric and gastroesophageal cancer. J Surg Oncol 2019; 120: 1350–1357. - PubMed
-
- Hayes T, Smyth E, Riddell A, Allum W. Staging in esophageal and gastric cancers. Hematol Oncol Clin North Am 2017; 31: 427–440. - PubMed
-
- Mezhir JJ, Shah MA, Jacks LMet al. . Positive peritoneal cytology in patients with gastric cancer: natural history and outcome of 291 patients. Ann Surg Oncol 2010; 17: 3173–3180. - PubMed
-
- Mirza A, Galloway S. Laparoscopy, computerised tomography and fluorodeoxyglucose positron emission tomography in the management of gastric and gastro-oesophageal junction cancers. Surg Endosc 2016; 30: 2690–2696. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous