

Treatment of Refractory Low Back Pain Using Passive Recharge Burst in Patients Without Options for Corrective Surgery: Findings and Results From the DISTINCT Study, a Prospective Randomized Multicenter Controlled Trial
- PMID: 37642628
- PMCID: PMC10801705
- DOI: 10.1016/j.neurom.2023.07.009
Treatment of Refractory Low Back Pain Using Passive Recharge Burst in Patients Without Options for Corrective Surgery: Findings and Results From the DISTINCT Study, a Prospective Randomized Multicenter Controlled Trial
Abstract
Objective: Spinal cord stimulation (SCS) is effective for relieving chronic intractable pain conditions. The Dorsal spInal cord STImulatioN vs mediCal management for the Treatment of low back pain study evaluates the effectiveness of SCS compared with conventional medical management (CMM) in the treatment of chronic low back pain in patients who had not undergone and were not candidates for lumbar spine surgery.
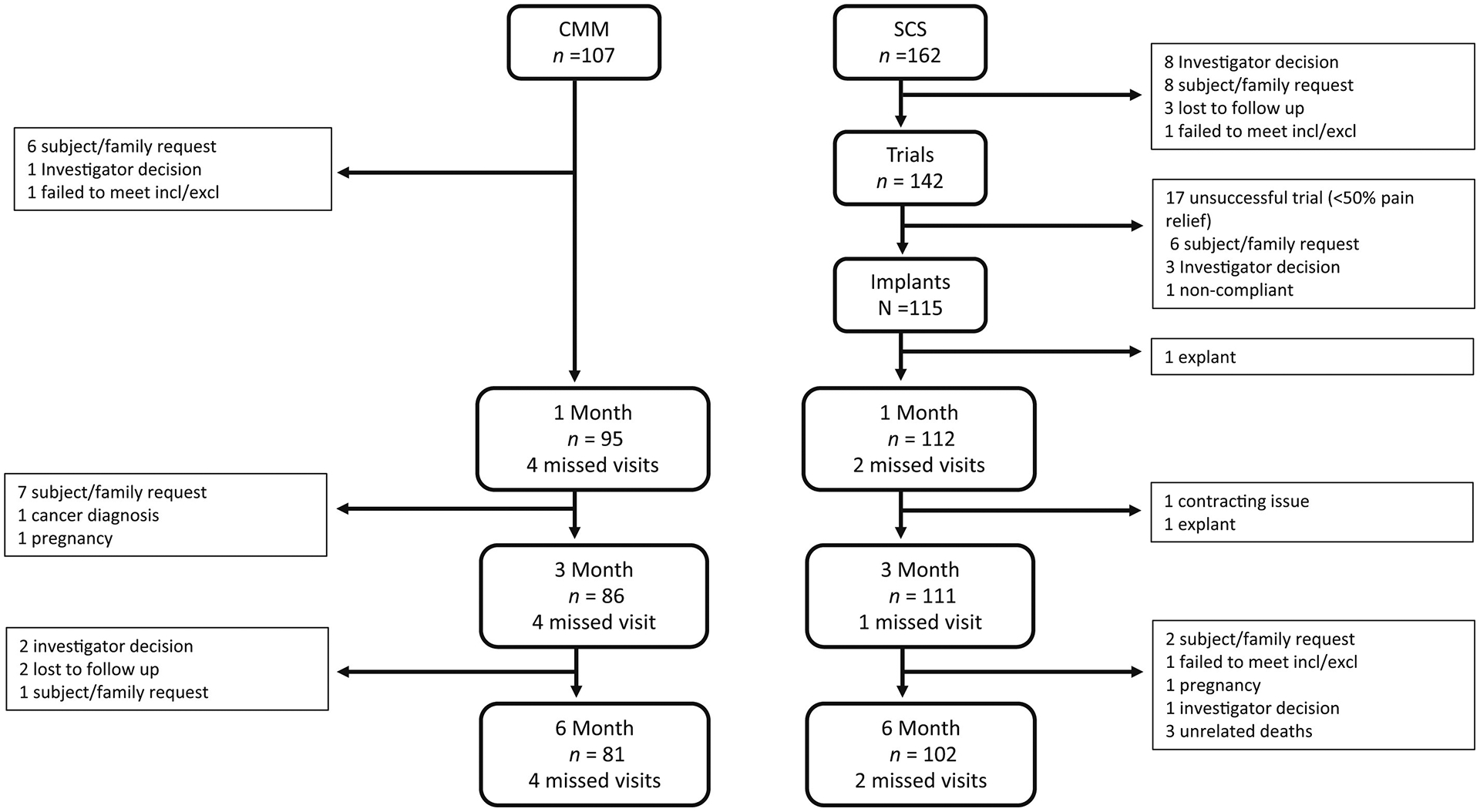
Methods and materials: Patients were randomized to passive recharge burst therapy (n = 162) or CMM (n = 107). They reported severe pain and disability for more than a decade and had failed a multitude of therapies. Common diagnoses included degenerative disc disease, spondylosis, stenosis, and scoliosis-yet not to a degree amenable to surgery. The six-month primary end point compared responder rates, defined by a 50% reduction in pain. Hierarchical analyses of seven secondary end points were performed in the following order: composite responder rate (numerical rating scale [NRS] or Oswestry Disability Index [ODI]), NRS, ODI, Pain Catastrophizing Scale responder rate, Patient Global Impression of Change (PGIC) responder rate, and Patient-Reported Outcome Measure Information System-29 in pain interference and physical function.
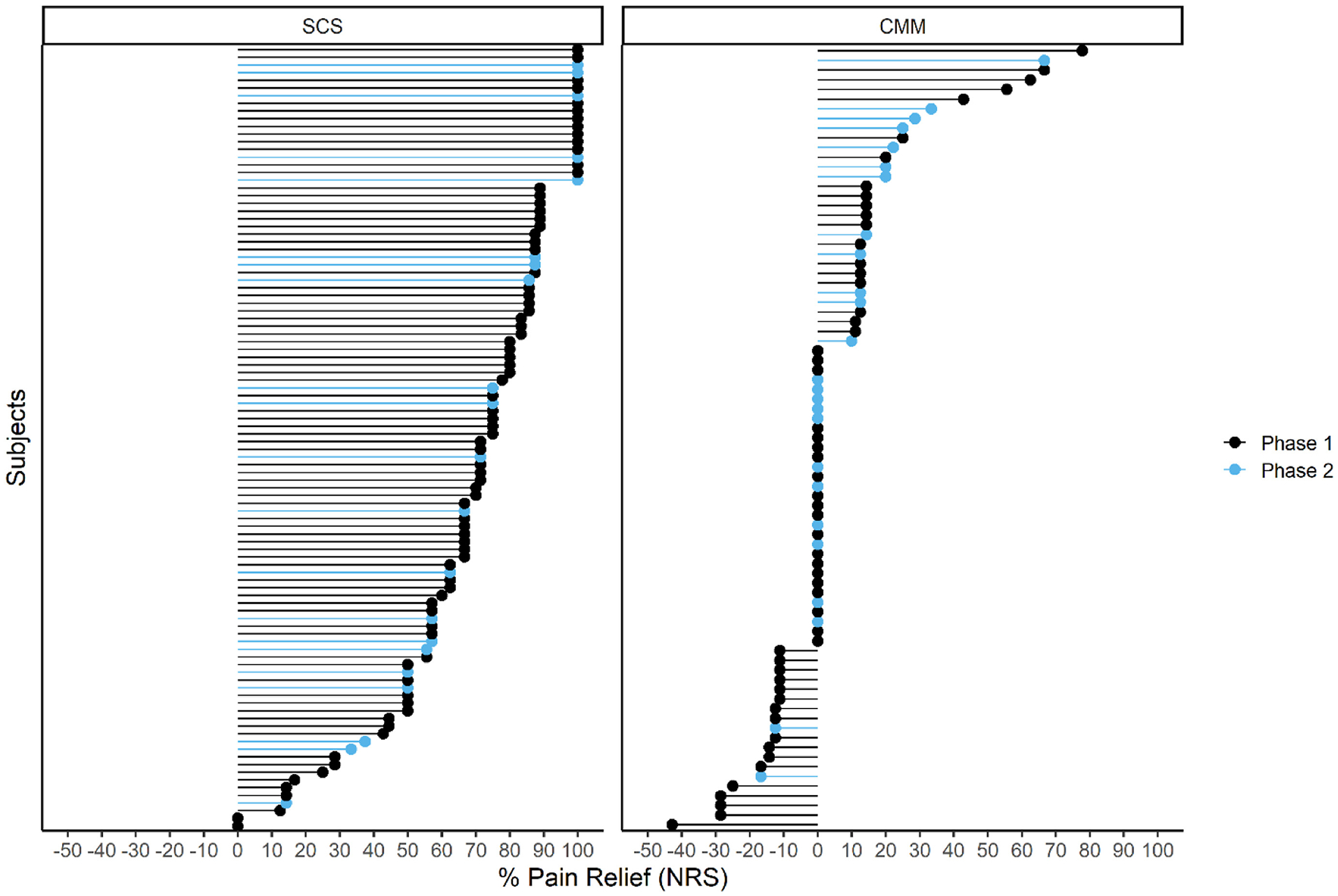
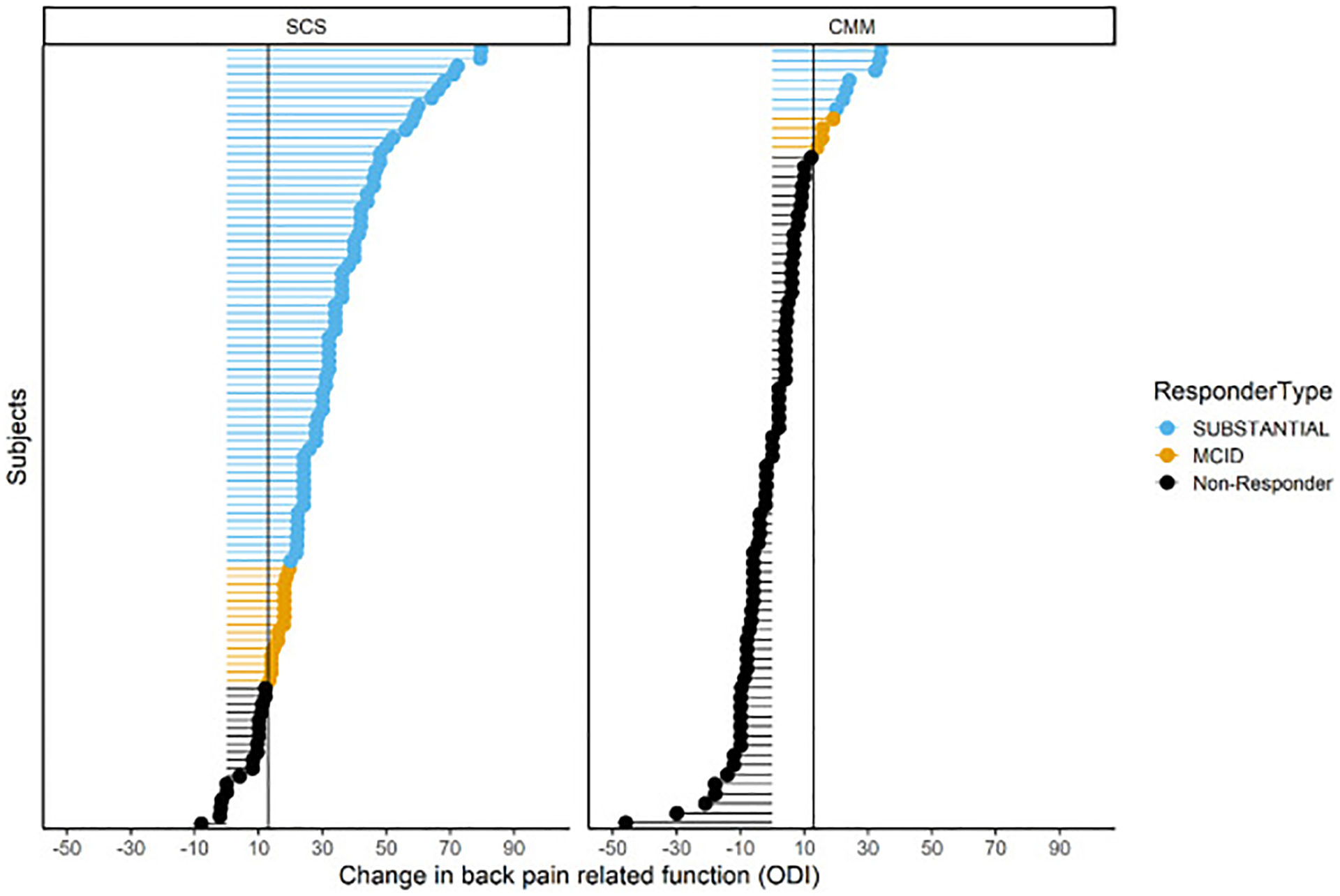
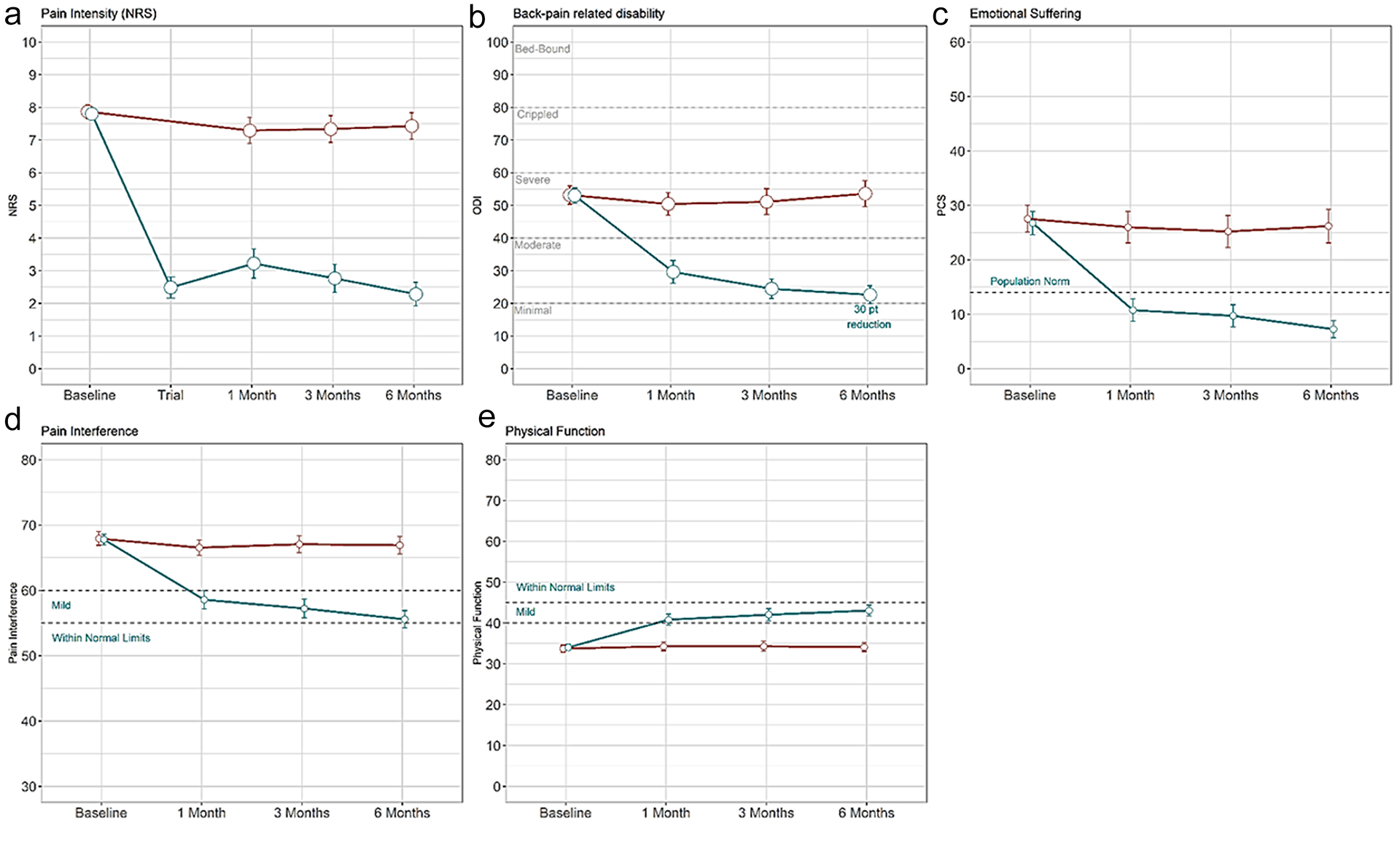
Results: Intention-to-treat analysis showed a significant difference in pain responders on NRS between SCS (72.6%) and CMM (7.1%) arms (p < 0.0001). Of note, 85.2% of those who received six months of therapy responded on NRS compared with 6.2% of those with CMM (p < 0.0001). All secondary end points indicated the superiority of burst therapy over CMM. A composite measure on function or pain relief showed 91% of subjects with SCS improved, compared with 16% of subjects with CMM. A substantial improvement of 30 points was observed on ODI compared with a <one-point change in the CMM arm. Three serious and 14 non-serious device- or procedure-related events were reported.
Conclusions: This study found substantial improvement at six months in back pain, back pain-related disability, pain-related emotional suffering, PGIC, pain interference, and physical function in a population with severe, debilitating back pain for more than a decade. These improvements were reported in conjunction with reduced opioid use, injection, and ablation therapy.
Clinical trial registration: The Clinicaltrials.gov registration number for the study is NCT04479787.
Keywords: composite outcomes; persistent spinal pain syndrome; refractory chronic low back pain; spinal cord stimulation.
Copyright © 2023 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest David Dickerson has a consulting relationship with Abbott Labs, Versos Medical, Biotronik, SPR Therapeutics, Pfizer, Nalu, and Myovant Biosciences. Robert M. Levy is an unpaid consultant for Abbott, Nalu, Biotronik and Saluda Medical. Robert M. Levy has stock options with Nalu and Saluda. Jacqueline Weisbein has consulting agreements with Abbott, Versos, Saluda, Biotronik and SI Bone. She has received payment or honoraria for lectures, presentations, speaking bureaus or educational events from Abbott and Saluda. Jacqueline Weisbein has received grants from Medtronic, Saluda, and SI Bone. Marie E. Fahey is an employee of Abbott. Denis Patterson has consulting agreements with Abbott, AIS, Allergan, Amgen, Pajunk Medical, Saluda, Aurora Spine, CornerLoc, Flowonix, Lundbeck, Spark Biomedical, and Versos and has received honoraria from Abbott, Allergan, Amgen, Vertos, CornerLoc, Lundbeck, and Saluda. He also has stock or stock options with CornerLoc. Julie Pilitsis has received grant support from Medtronic, Boston Scientific, and Abbott. Timothy Deer has consulting agreements with Abbott, Saluda, Nalu, and SPR Therapeutics and has received grant support from Saluda, Nalu, and SPR Therapeutics. Timothy Deer has stocks or stock options with Saluda, Nalu, and SPR Therapeutics. Steven Falowski has consulting agreements with Medtronic, Abbott, Saluda, Vertos, CornerLoc, Mainstay Medical, Relievant, and Avanos and has received grant support from Abbott, Mainstay, Medtronic, Vertiflex, CornerLoc, Saluda, Nalu, and Biotronik. He also has stocks or stock options with SPR Therapeutics, Saluda and Stimgenics. Ajay Antony has consulting agreements with Abbott, Boston Scientific, Saluda, Versos, PainTEQ, and Avanos and serves on an advisory board for Boston Scientific, Abbott, and Saluda. Patrick Buchanan reports consulting fees from Abbott and PainTEQ. Mehul Desai reports consulting fees from Abbott, SPR Therapeutics and Nalu Medical and stock or stock options from SPR Therapeutics, Synerfuse, Virdio, and VYRSA. Chris Gilligan reports consulting fees from Mainstay Medical, Persica, Saluda, and Iliad Lifesciences and stock or stock options from Mainstay Medical. Robert Heros reports consulting fees from Abbott, Mainstay Medical, Saluda Medical, Biotronik, and Boston Scientific and support for attending meetings from Mainstay Medical and participated on a data safety monitoring board/advisory board for Biotronik. Jessica Jameson reports consulting fees from Boston Scientific, Nevro, Saluda, Abbott, and SI Bone and payment or honoraria from Nevro, Boston Scientific, Saluda, Abbott, and Medtronic. Chi Lim reports consulting fees from Synthes, Medtronic, Abbott, Implanet, Kyocera, and Met One. Derron Wilson reports consulting fees from Abbott, Boston Scientific and Biotronik and payment or honoraria for lectures, or educational events from Abbott and has received travel support from Abbott, Biotronik, and Boston Scientific. Derron Wilson has participated on advisory boards for Abbott and Biotronik. James J. Yue reports consulting income and grant support from Abbott. Susan Moeschler, Jijun Xu, Edward Braun, Kenneth Candido, Anne Christopher, Jonathan Duncan, Michael Fishell, Robert Funk, Mohab Ibrahim, Scott Kreiner, Nathan Miller, Keith-Austin Scarfo, Edward Tavel, and Sayed Wahezi reported no conflict of interest.
Figures
References
-
- Hoy D, Bain C, Williams G, et al. A systematic review of the global prevalence of low back pain. Arthritis Rheum. 2012;64:2028–2037. - PubMed
-
- Kreiner DS, Matz P, Bono CM, et al. Guideline summary review: an evidence-based clinical guideline for the diagnosis and treatment of low back pain. Spine J. 2020;20:998–1024. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
