

Closure rates and patterns after light silicone oil tamponade for persistent full-thickness macular holes
- PMID: 37642749
- PMCID: PMC10667392
- DOI: 10.1007/s00417-023-06215-w
Closure rates and patterns after light silicone oil tamponade for persistent full-thickness macular holes
Abstract
Purpose: To report outcomes of re-vitrectomy using light silicone oil (SO) tamponade for persistent macular holes (MHs).
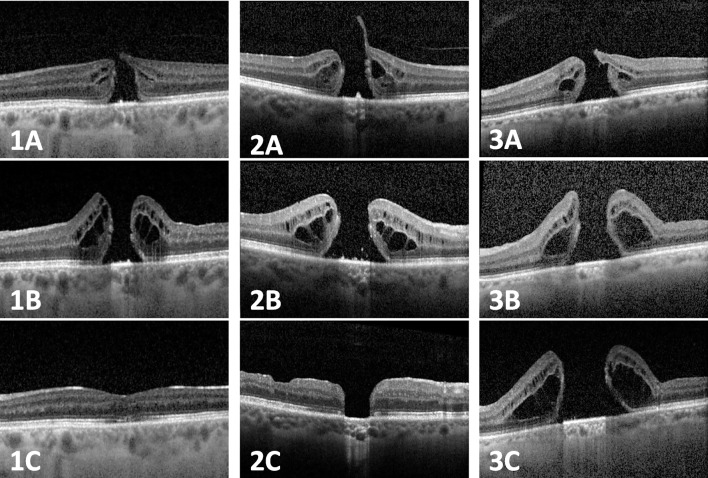
Methods: We reviewed cases of patients with full-thickness MHs that underwent pars plana vitrectomy (PPV) with air/gas and were re-vitrectomized using light SO tamponade after primary non-closure (persistent MHs). Outcome measures included anatomic closure rates and patterns confirmed by optical coherence tomography (OCT) and changes in best-corrected visual acuity (BCVA).
Results: A total of 42 eyes of 41 patients with unsuccessful primary PPV with air/gas were included. After re-vitrectomy with light SO (1000-centistoke), 29 (69%) eyes demonstrated type 1 closure without neurosensory defects in OCT scans, whereas 9 eyes (21%) showed type 2 closure with persisting neurosensory defects. Available data (n = 21) showed a significant mean improvement of BCVA from 0.99 logMAR (SD 0.25, range 0.7-1.3) preoperatively to 0.74 logMAR (SD 0.42, range 0.2-1.5) postoperatively (p = 0.035).
Conclusion: The treatment of persistent MHs with PPV and light SO tamponade resulted in high closure rates.
Keywords: Pars plana vitrectomy; Persistent macular hole; Refractory macular hole; Silicone oil.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no copmeting interests.
Figures
Similar articles
-
Surgical treatment and optical coherence tomographic evaluation for accidental laser-induced full-thickness macular holes.Eye (Lond). 2017 Jul;31(7):1078-1084. doi: 10.1038/eye.2017.41. Epub 2017 Mar 10. Eye (Lond). 2017. PMID: 28282068 Free PMC article.
-
Outcome of autologous platelet concentrate and gas tamponade compared to heavy silicone oil tamponade in persistent macular hole surgery.Eur J Ophthalmol. 2021 Mar;31(2):664-672. doi: 10.1177/1120672120903704. Epub 2020 Feb 4. Eur J Ophthalmol. 2021. PMID: 32019342
-
Silicone oil tamponade for persistent macular holes.Eye (Lond). 2021 Aug;35(8):2206-2212. doi: 10.1038/s41433-020-01228-9. Epub 2020 Oct 21. Eye (Lond). 2021. PMID: 33087884 Free PMC article.
-
Pars plana vitrectomy with internal limiting membrane flap versus pars plana vitrectomy with conventional internal limiting membrane peeling for large macular hole.Cochrane Database Syst Rev. 2023 Aug 7;8(8):CD015031. doi: 10.1002/14651858.CD015031.pub2. Cochrane Database Syst Rev. 2023. PMID: 37548231 Free PMC article. Review.
-
Pars plana vitrectomy with silicone oil tamponade for primary and secondary macular hole closure: Is it still a useful procedure?Eur J Ophthalmol. 2018 Sep;28(5):503-514. doi: 10.1177/1120672117752423. Epub 2018 Mar 19. Eur J Ophthalmol. 2018. PMID: 30246566 Review.
Cited by
-
[Macular hole: Differential diagnosis, treatment options and new guideline recommendations].Ophthalmologie. 2024 Jun;121(6):462-469. doi: 10.1007/s00347-024-02047-z. Epub 2024 May 22. Ophthalmologie. 2024. PMID: 38775987 Review. German.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
